|


 |
| CASE REPORT |
|
| Year : 2013 | Volume
: 5
| Issue : 1 | Page : 27-31 |
|
|
Pneumobilia: A case report and literature review on its surgical approaches
Chee Siong Wong1, James Maurice Crotty2, Syed Altaf Naqvi3
1 Royal College of Surgeons in Ireland, Dublin, Ireland
2 Department of Radiology, Limerick University Hospital, Limerick, Co. Limerick, Ireland
3 Department of Surgery, Limerick University Hospital, Limerick, Co. Limerick, Ireland
| Date of Web Publication | 21-Sep-2013 |
Correspondence Address:
Chee Siong Wong
Royal College of Surgeons in Ireland, Dublin
Ireland
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.118616

 Abstract Abstract | | |
Gallstones ileus is an uncommon cause but important cause of small bowel obstruction. The gallstone enters the intestinal lumen via a fistula located in the duodenum (cholecystoduodenal), or rarely, in the colon (cholecystocolonic) or stomach (cholecystogastric). This may result in large bowel or gastric outlet obstruction (Bouveret's Syndrome). Gallstone ileus affects the elderly females pre-dominantly and is associated with a high morbidity and mortality rate if diagnosis and urgent surgical intervention are delayed. In this paper, we report on the case of an elderly lady who presented with classical symptoms and signs of small bowel obstruction. She was subsequently diagnosed with gallstone ileus due to a large gallstones lodged in the intestinal lumen. We perform a literature review on this rare disease and discuss the two main surgical approaches in managing this condition. Gallstone ileus should be considered in the differential diagnosis of small bowel obstruction especially in elderly women who have no history of abdominal surgery or abdominal hernia. Early intervention is important because of the high mortality rate due to the poor general condition that often exists in this subgroup of patients. There is no general consensus on gold standard surgical approach in these cases but a two-stage procedure (either enterotomy alone or enterotomy and subsequent cholecystectomy) has been shown to be associated with lower mortality rates. Keywords: Gallstone ileus, pneumobilia, rigler′s triad, small bowel obstruction
How to cite this article:
Wong CS, Crotty JM, Naqvi SA. Pneumobilia: A case report and literature review on its surgical approaches. J Surg Tech Case Report 2013;5:27-31 |
How to cite this URL:
Wong CS, Crotty JM, Naqvi SA. Pneumobilia: A case report and literature review on its surgical approaches. J Surg Tech Case Report [serial online] 2013 [cited 2016 May 25];5:27-31. Available from: http://www.jstcr.org/text.asp?2013/5/1/27/118616 |
| Introduction | |  |
Gallstones ileus is defined as mechanical intestinal obstruction caused by a large gallstone lodged in the bowel lumen. This condition accounts for only 1% of case with small bowel obstructions and 2% of patients with gallstone disease. It is uncommon but it is seen most often in women and the elderly population which accounts for up to 20% in the latter group. The pathophysiology of gallstone ileus is related to the formation of cholecystoenteric fistula which allows gallstones to enter the intestinal lumen. Most (75%) of these fistulas develop between the gallbladder and duodenum, although it is possible that the gallstone gains entry to the duodenum via a fistula with the biliary tract.
Patients with gallstone ileus may have a history of gallbladder-related symptoms without previous surgery or hernia on physical examination. They usually present with acute intestinal obstruction, either partial or complete, depending on the size of the stone. Classically, the stones are almost always 2.5 cm or more in diameter and can be found impacted at about 60 cm proximal to ileocaecal valve.
Abdominal radiograph findings include dilated small bowel, the presence of gas in the biliary system (pneumobilia), and a gallstone in the right iliac fossa. Although pneumobilia is one of the radiological features of gallstones ileus, other conditions may also demonstrate this finding, including incompetent Sphincter of Oddi More Details, [1] infection of the gallbladder (emphysematous cholecystitis), [2],[3] and rarely gallbladder cancer [4] and blunt trauma. [5],[6],[7]]
The initial management of gallstone ileus is to relieve the bowel obstruction by performing a small enterotomy. The proximal intestine should be carefully inspected for a second calculus. The bowel is also inspected for any evidence of ischemic bowel with resection of any infracted segments. In patients who can tolerate it, cholecystectomy is also performed at the same time as the enterotomy. Otherwise, an elective cholecystectomy can be performed at a later date. The cholecystoduodenal fistula itself closes spontaneously in the majority of patients.
| Case Report | | |
An 82-year-old woman presented to the emergency department with a 1 week history of vomiting, mild abdominal discomfort, and absolute constipation. The latter was preceded by gradual worsening of bile-stained non-projectile vomiting. She denied any fever or urinary symptoms. She was a type 2 diabetic and had a history of hypertension. She had no previous abdominal surgery. She was a non-smoker and denied recent alcohol consumption. On physical examination, she was apyrexial, pulse rate was 78 beats per minute, blood pressure was 110/60 mmHg, and respiratory rate was 25 breaths per minute. Her abdomen was soft and non-distended, but there was mild generalized tenderness elicited on palpation. There was no guarding or rebound tenderness. No obvious inguinal or femoral hernia on clinical examination. Digital rectal examination was unremarkable.
Laboratory tests were as follows: White Blood Cells, 16.55 × 10 9 /L; Hb, 14.1 g/dl; Platelet, 387 10 9 /L × 10 9 /L; Na, 118 mmol/L; K, 2.8 mmol/L; urea, 16.1 mmol/L; creatinine, 101 mmol/L; bilirubin (total), 18 μmol/L; alkaline phosphatase, 72 IU/L; and amylase, 69 IU/L. The arterial blood gas measurement suggested a hypochloremic metabolic alkalosis (pH 7.55, pCO 2 6.17 kPa, bicarbonate 39.5 mmol/L, chloride 68 mmol/L, and lactate 1.7 mmol/L). Urine dipstick was negative for glucose, bilirubin, ketone, blood, protein, nitrates, and leukocytes.
An erect chest radiograph was normal with no evidence of subdiaphragmatic air [Figure 1]. Abdominal radiograph showed dilated small bowel loop in the central of abdomen [Figure 2]. For a detailed evaluation of the level of bowel obstruction, a contrast computed tomography (CT) of the abdomen and pelvis was requested. CT examination of the abdomen and pelvis showed findings consistent with proximal small bowel obstruction, pneumobilia located in the right hepatic lobe [Figure 3], and a gallstone in the distal small bowel [Figure 4]. These features strongly suggested the diagnosis of gallstone ileus.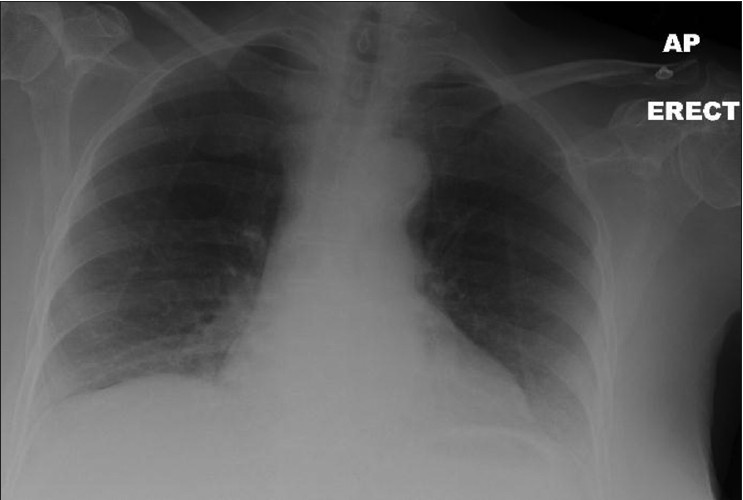 | Figure 1: An erect chest radiograph: No evidence of air beneath the diaphragm
Click here to view |
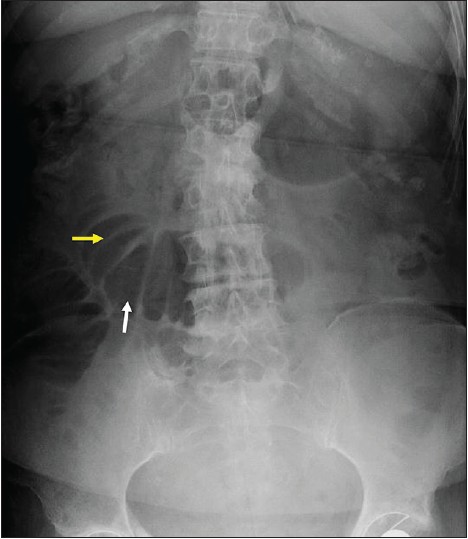 | Figure 2: Abdominal radiograph: Central, dilated loops of small bowel (white arrow). Note the plicae circulares or valvulae conniventes (yellow arrow), a feature of small bowel, which confirms that the dilated structure is small bowel. Some loops measure 64 mm in diameter. There is no gas within the large bowel suggesting a complete or nearly complete mechanical small bowel obstruction
Click here to view |
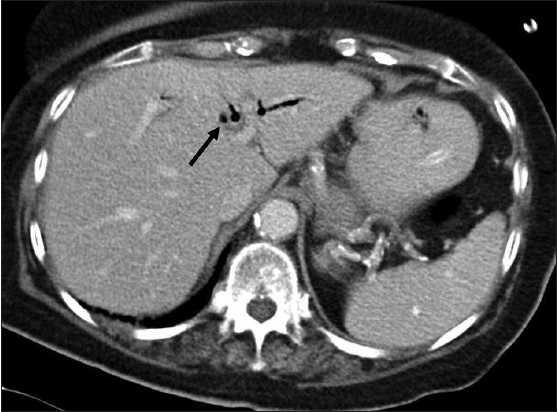 | Figure 3: Axial CT image of the upper abdomen: There is diffuse pneumobilia (black arrow)
Click here to view |
 | Figure 4: Axial CT image of the pelvis: There is a calculus (white arrow) identified within the small bowel lumen. Note the presence of both dilated and non‑dilated small bowel
Click here to view |
After initial fluid resuscitation with 0.9% sodium chloride, correction of electrolyte imbalance, and nasogastric decompression, the patient underwent midline laparotomy. A proximal longitudinal enterotomy was performed. Numerous small bowel stones [Figure 5] of variable size were "milked" distally. The largest stone measured 3.5 cm in diameter was retrieved from the small bowel lumen [Figure 6]. Each section of the bowels was inspected in a segmental fashion for sign of ischemia and other intra-luminal faceted gallstones. An abdominal washout was performed using warm saline in order to prevent gross peritoneal contamination. The abdominal incision was closed by a mass closure technique using an absorbable loop Maxon TM suture and staples to the skin. The fistula was left undisturbed and the patient made an uneventful recovery.
| Discussion | | |
Gallstone ileus is an uncommon complication of cholelithiasis and cholecystitis. It is responsible for less than 1% of all cases of small bowel obstruction. The pathophysiology of formation of a fistula is associated with chronic inflammation of the gallbladder.
The clinical symptoms of gallstone ileus are often non-specific. A typical history of gallstone ileus is an intermittent and episodic abdominal complaint as the calculus passes down the intestinal tract. This phenomenon is called a "tumbling obstruction." Diagnosis of this rare condition should be suspected in the elderly who presented with symptoms and sign of bowel obstruction without a history of previous abdominal surgery or hernia on physical examination.
A plain abdominal radiograph may show dilatation of small bowel (small bowel obstruction), air in the biliary tree (pneumobilia), and opacity in the right iliac fossa (ectopic gallstone). The feature of small bowel obstruction, pneumobilia, and ectopic gallstone represents Rigler's triad which is consistent with a diagnosis of gallstone ileus. [8] The triad presents only 14.81% on plain film of the abdomen, 11.11% on abdominal sonography, and 77.78% on abdominal CT scan. [9] This is not surprising because plain abdominal radiograph reveals radio opaque gallstones in only 10% of cases. In the latter study, it was shown that pneumobilia can be detected up to 89% of all cases of gallstone ileus. [9] In the past, the diagnosis was often made during laparotomy. [10] Plain abdominal radiography and ultrasound are helpful in diagnosing gallstone ileus but the sensitivity of both modalities is low. CT scan is the investigation of choice for evaluating gallstone ileus as it has high sensitivity (93%) and specificity (100%). A CT scan can accurately measure the size of the gallstone and establish the anatomical site and the nature of the obstruction. Comparison between specificity and sensitivity of each modality is shown in [Table 1] . Therefore, CT scan is usually a preferred diagnostic modality because of its high resolution in detecting gallstones and provides details of anatomical localization of the gallstone and fistula.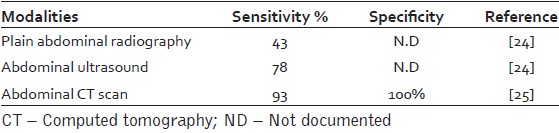 | Table 1: Sensitivity and specificity of different modalities in diagnosing gallstone ileus
Click here to view |
The initial management of gallstone ileus is to relieve the obstruction by removing the gallstone through a proximal enterotomy. Spontaneous resolution of symptoms of gallstone ileus has been reported but uncommon. [11] At present, the mainstay of treatment for gallstone is surgical. The choice of a one-stage or two-stage surgical procedure or enterotomy alone is still debatable.
The reported mortality rates of gallstone ileus are generally consistent at about 20% for the first time ileus presentation [12] and at subsequent recurrent episodes. [13] It is therefore important to establish early diagnosis and initiate prompt surgical treatment. Most of the retrospective studies conducted so far suggested that higher mortality rates were observed in the one-stage procedure [Table 2]. To date, the largest single published review of this condition, by Reisner and Cohen found that one-stage procedure carries higher risk of mortality compared to simple enterotomy. [10] Associated factors of a higher mortality rate may attribute to: (1) Pre-operatively, (2) Intra-operatively, and (3) Post-operatively. First, pre-operatively: Elderly patients with poor general medical conditions, delayed diagnosis, and prompt treatment of this uncommon condition as well as inadequate physiological state optimization pre-operatively prior to the time of emergency laparotomy may result in a poorer surgical outcome. Second, intra-operatively: Longer operating time for the one-stage procedure may lead to higher mortality. Third, post-operatively: Deaths may not be related to the surgery, for example, myocardial infarction or pulmonary embolism.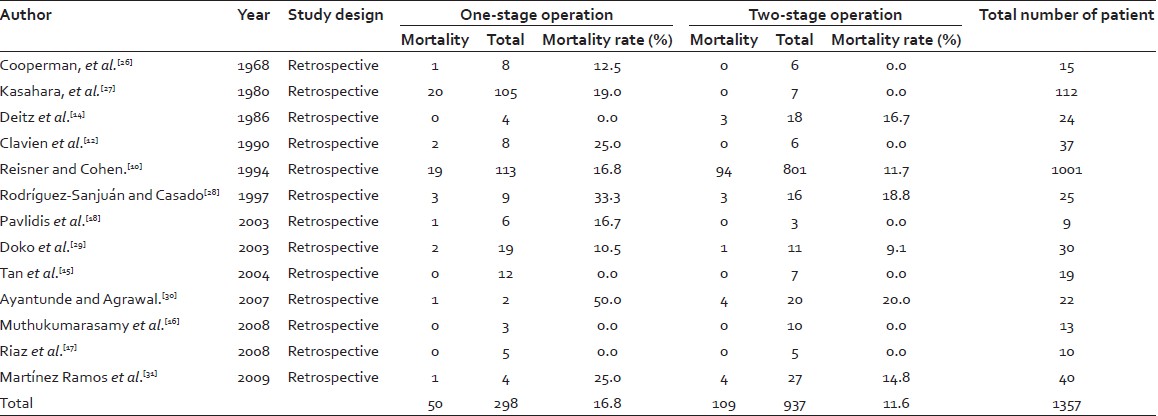 | Table 2: Comparison of mortality rates of two main surgical approaches in treating gallstone ileus, one‑stage and two‑stage procedure
Click here to view |
In this brief report, we compared mortality rates of the two main surgical approaches, one-stage procedure (comprising enterotomy, cholecystectomy, and fistula repair) and two-stage procedure (enterotomy with or without subsequent cholecystectomy and fistula repair). There is no general consensus on "gold standard" surgical intervention and the controversy of these is still remaining arguable. Of all selected 13 studies that provide adequate data comparing mortality rates in one-stage and two-stage procedures, we found a higher mortality rate in one-stage procedure (16.8%) compared to two-stage procedure (11.8%). Surprisingly, the results from these collective studies are similar to the previously reported data by Reisner and Cohen. [10] A majority of the studies observed higher mortality rates in one-stage procedure except Deitz et al. The author observed a higher mortality rate in two-stage procedure (16.7%). [14] Some authors did not find any differences between the two groups of surgical intervention. [15],[16],[17]
Pavlidis et al., selectively performed two-stage operation for all patients with American Society of Anesthesiologists (ASA) score three or more. He observed no mortality in this group. [18] The author reserved one-stage procedure for relatively good ASA score patient. He concluded that two-stage procedure should be performed in patients with unfavorable ASA score.
Laparoscopic procedures do not represent gold standard treatment for gallstone ileus. One can argue that laparoscopy increases operative time of the surgery due to technical difficulty finding the gallstone and requires specialist trained surgeons. On the other hand, laparoscopy inflicts less operative trauma on the patient, which may result in less morbidity and mortality. Some recent reports have been published on the efficacy of the laparoscopic approach in the management of gallstone ileus. To date, there are five studies [19],[20],[21],[22],[23] regarding the use of laparoscopy in the treatment of gallstone ileus. There is no mortality reported. These reports demonstrate that laparoscopy is effective in both diagnosis and treatment of gallstone ileus. The number of patients in each study is small; therefore, we do not have enough clinical data to allow comparison between one-stage and two-stage procedures performed laparoscopically.
| Conclusion | | |
Gallstone ileus is a rare complication of gallstone disease. It carries high mortality rates in elderly. Therefore, a prompt diagnosis followed by urgent optimization of patient prior to appropriate surgical intervention is essential. A two-stage procedure should be considered in all elderly patients with significant co-morbidities. A one-stage procedure, on the other hand, should be reserved for young, fit, and low-risk patient with a favorable ASA score.[31]
| References | | |
| 1. | Broadman SA. Incompetence of the sphincter of Oddi: An uncommon cause of pneumobilia: Report of a case. J Am Osteopath Assoc 1971;70:565-9. 
[PUBMED] |
| 2. | Ohtani Y, Tanaka Y, Tsukui M, Goto K, Moriya H, Tobita K, et al. Acute emphysematous cholecystitis associated with pneumobilia: A case report. Tokai J Exp Clin Med 1996;21:33-6.
[PUBMED] |
| 3. | Lin YF, Chao HM, His SC. Emphysematous cholecystitis with pneumobilia. Dig Surg 2009;26:20-1.
[PUBMED] |
| 4. | Dadzan E, Akhondi H. Choledochoduodenal fistula presenting with pneumobilia in a patient with gallbladder cancer: A case report. J Med Case Rep 2012;6:61.
|
| 5. | Gering SA, Foster MA, Harnisch MC, McNeil JJ. Traumatic pneumobilia: Case report. J Trauma 2001;51:391-4.
[PUBMED] |
| 6. | Thompson RJ, Irwin T. Pneumobilia following blunt abdominal trauma. Ir J Med Sci 2007;176:313-5.
[PUBMED] |
| 7. | Yildiz F, Coban S, Terzi A, Cece H, Uzunkoy A. An uncommon cause of pneumobilia: Blunt abdominal trauma. Ulus Travma Acil Cerrahi Derg 2011;17:363-4.
|
| 8. | Rigler LG, Broman CN, Broman JF. Gallstone Obstruction: Pathogenesis and roentgen manifestation. JAMA 1941;117:1753-9.
|
| 9. | Lassandro F, Gagliardi N, Scuderi M, Pinto A, Gatta G, Mazzeo R. Gallstone ileus analysis of radiological findings in 27 patients. Eur J Radiol 2004;50:23-9.
[PUBMED] |
| 10. | Reisner RM, Cohen JR. Gallstone ileus: A review of 1001 reported cases. Am Surg 1994;60:441-6.
[PUBMED] |
| 11. | Farooq A, Memon B, Memon MA. Resolution of gallstone ileus with spontaneous evacuation of gallstone. Emerg Radiol 2007;14:421-3.
[PUBMED] |
| 12. | Clavien PA, Richon J, Burgan S, Rohner A. Gallstone ileus. Br J Surg 1990;77:737-42.
[PUBMED] |
| 13. | Guttikonda S, Vaswani KK, Vitellas KM. Recurrent gallstone ileus: A case report. Emerg Radiol 2002;9:110-2.
[PUBMED] |
| 14. | Deitz DM, Standage BA, Pinson CW, McConnell DB, Krippaehne WW. Improving the outcome in gallstone ileus. Am J Surg 1986;151:572-6.
[PUBMED] |
| 15. | Tan YM, Wong WK, Ooi LL. A comparison of two surgical strategies for the emergency treatment of gallstone ileus. Singapore Med J 2004;45:69-72.
[PUBMED] |
| 16. | Muthukumarasamy G, Venkata SP, Shaikh IA, Somani BK, Ravindran R. Gallstone ileus: Surgical strategies and clinical outcome. J Dig Dis 2008;9:156-61.
[PUBMED] |
| 17. | Riaz N, Khan MR, Tayeb M. Gallstone ileus: Retrospective review of a single centre›s experience using two surgical procedures. Singapore Med J 2008;49:624-6.
[PUBMED] |
| 18. | Pavlidis TE, Atmatzidis KS, Papaziogas BT, Papaziogas TB. Management of gallstone ileus. J Hepatobiliary Pancreat Surg 2003;10:299-302.
[PUBMED] |
| 19. | Montgomery A. Laparoscope-guided enterolithotomy for gallstone ileus. Surg Laparosc Endosc 1993;3:310-4.
[PUBMED] |
| 20. | Franklin ME Jr, Dorman JP, Schuessler WW. Laparoscopic treatment of gallstone ileus: A case report and review of the literature. J Laparoendosc Surg 1994;4:265-72.
[PUBMED] |
| 21. | Sarli L, Pietra N, Costi R, Gobbi S. Gallstone ileus: Laparoscopic-assisted enterolithotomy. J Am Coll Surg 1998;186:370-1.
[PUBMED] |
| 22. | Soto DJ, Evan SJ, Kavic MS. Laparoscopic management of gallstone ileus. JSLS 2001;5:279-85.
[PUBMED] |
| 23. | Zygomalas A, Karamanakos S, Kehagias I. Totally laparoscopic management of gallstone ileus: Technical report and review of the literature. J Laparoendosc Adv Surg Tech A 2012;22:265-8.
[PUBMED] |
| 24. | Ripollés T, Miguel-Dasit A, Errando J, Morote V, Gómez-Abril SA, Richart J. Gallstone ileus: Increased diagnostic sensitivity by combining plain film and ultrasound. Abdom Imaging 2001;26:401-5.
|
| 25. | Yu CY, Lin CC, Shyu RY, Hsieh CB, Wu HS, Tyan YS, et al. Value of CT in the diagnosis and management of gallstone ileus. World J Gastroenterol 2005;11:2142-7.
[PUBMED] |
| 26. | Cooperman AM, Dickson ER, ReMine WH. Changing concepts in the surgical treatment of gallstone ileus: A review of 15 cases with emphasis on diagnosis and treatment. Ann Surg 1968;167:377-83.
[PUBMED] |
| 27. | Kasahara Y, Umemura H, Shiraha S, Kuyama T, Sakata K, Kubota H. Gallstone ileus. Review of 112 patients in the Japanese literature. Am J Surg 1980;140:437-40.
[PUBMED] |
| 28. | Rodríguez-Sanjuán JC, Casado F, Fernández MJ, Morales DJ, Naranjo A. Cholecystectomy and fistula closure versus enterolithotomy alone in gallstone ileus. Br J Surg 1997;84:634-7.
|
| 29. | Doko M, Zovak M, Kopljar M, Glavan E, Ljubicic N, Hochstädter H. Comparison of surgical treatments of gallstone ileus: Preliminary report. World J Surg 2003;27:400-4.
|
| 30. | Ayantunde AA, Agrawal A. Gallstone ileus: Diagnosis and management. World J Surg 2007;31:1292-7.
[PUBMED] |
| 31. | Martínez Ramos D, Daroca José JM, Escrig Sos J, Paiva Coronel G, Alcalde Sánchez M, Salvador Sanchís JL. Gallstone ileus: Management options and results on a series of 40 patients. Rev Esp Enferm Dig 2009;101:117-20, 121-4.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6]
[Table 1], [Table 2]
|

















