|


 |
| CASE REPORT |
|
| Year : 2013 | Volume
: 5
| Issue : 1 | Page : 48-50 |
|
|
Vesical calculus 10 years post missing intrauterine contraceptive device
Abdullahi Abdulwahab-Ahmed, Oluwagbemiga Olabisi Ogunleye
Department of Surgery, Usmanu Danfodiyo University, Teaching Hospital, Sokoto, Nigeria
| Date of Web Publication | 21-Sep-2013 |
Correspondence Address:
Abdullahi Abdulwahab-Ahmed
Department of Surgery, Usmanu Danfodiyo University, Teaching Hospital, Sokoto
Nigeria
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.118630

 Abstract Abstract | | |
Intravesical migration of intrauterine contraceptive device (IUCD) is rare. Early diagnosis of this rare entity is difficult because of its non-specific manifestations and very low index of suspicion. We present this case of bladder stone following intravesical migration of IUCD found to have been missing since insertion 10 years earlier. Lower abdominal discomfort and a missing vaginal string may be the only pointer to this unfortunate event in the immediate post insertion period. It is pertinent to consider the possibility of an intravesical migration of a missing IUCD in a patient presenting with lower abdominal discomfort, urinary frequency, and missing IUCD string on vaginal examination. Keywords: Bladder stone, intrauterine contraceptive device, intravesical migration
How to cite this article:
Abdulwahab-Ahmed A, Ogunleye OO. Vesical calculus 10 years post missing intrauterine contraceptive device. J Surg Tech Case Report 2013;5:48-50 |
How to cite this URL:
Abdulwahab-Ahmed A, Ogunleye OO. Vesical calculus 10 years post missing intrauterine contraceptive device. J Surg Tech Case Report [serial online] 2013 [cited 2016 May 25];5:48-50. Available from: http://www.jstcr.org/text.asp?2013/5/1/48/118630 |
| Introduction | |  |
Intrauterine contraceptive devices (IUCD) are acceptable means of contraception world over. [1],[2],[3],[4] There have been reports of its migration to other adjourning sites in the body after proper and satisfactory insertion into the uterine cavity. [5] Difficult intrauterine placement of IUCD and eventful immediate post insertion period could be the only pointer to inappropriate placement at insertion. We present this unique case of vesical stone formed on and around an IUCD placed 10 years earlier in a woman who had an eventful IUCD insertion; in an attempt to emphasize the need to look for a missing device in the urinary bladder.
| Case Report | | |
A 43-year-old teacher para 5 + 0 five alive presented to our clinic with a year history of recurrent lower abdominal pain, irritative lower urinary tract symptoms (LUTS) and strangury. There was no obstructive LUTS. Four weeks before her presentation to us, she developed hematuria initially terminal, but a day to presentation became total. There was no syncope and no easy fatigue. There were no other constitutional symptoms.
Ten years ago, she had IUCD in the form of Copper T inserted for contraception. The procedure of insertion was eventful with difficulty in intrauterine placement of the device, lower abdominal discomfort, and urinary frequency after the procedure. She re-presented at the contraceptive clinic 24 h after insertion due to unbearable lower abdominal pain. This was relieved by oral analgesics. The IUCD string; however was not seen at vaginal examination during this visit to contraceptive clinic, and the IUCD was not sought for any further. She remains relatively symptoms free until a year prior to presentation.
On examination, there was no abnormality found. Abdominal ultrasound reported vesical calculus and pelvic X-ray confirmed stone [Figure 1]. Other laboratory results were within normal limits.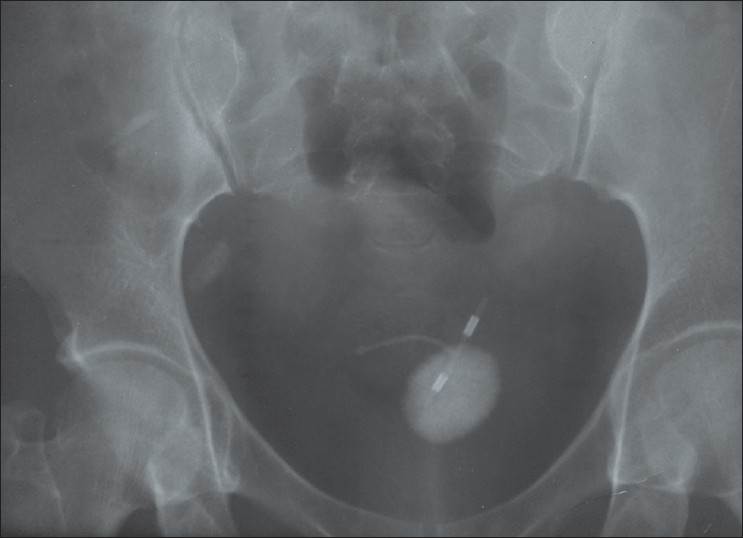 | Figure 1: Pelvic X‑ray showing bladder stone with embedded Copper T intrauterine contraceptive device
Click here to view |
She had open cystolithotomy with retrieval of stone encrusted Copper T IUCD [Figure 2], she did well and has been symptoms and stone free afterward.
| Discussion | | |
There are many complications of an IUCD; these include menorrhagia, hypermenorrhea, dysmenorrhea, pelvic inflammatory disease, spontaneous abortion, unwanted pregnancy, uterine perforation, and migration. [2],[5] These complications are rare and are the usual indication of IUCD removal. Despite these reported complications of IUCD, it is still accepted world-wide as contraceptive agent. Intravesical migration of IUCD with subsequent stone formation around it is one of the rarest complications of IUCD. [2],[3],[4]
Vesical stone are uncommon in female and are mostly seen in patients with infravesical obstruction especially from genital prolapse or after surgery for correction of incontinence. [6],[7] Secondary bacterial infection of urine with urease forming organism results in stone formation in these group of patients. Foreign body in the bladder can serve as a nidus for stone formation. [7],[8] In this patient, the nidus for stone concretion is the IUCD that migrated into the bladder. The presence of foreign body in the bladder may present with a little or no symptoms in the initial period, but as a complication of its presence in the bladder develops, irrtative LUTS become apparent and progressively worsen. [9],[10],[11],[12],[13] With infection and encrustation around it subsequently there is stone formation. Soon there is the development of both irritative and obstructive LUTS and hematuria [10],[14],[15] from recurrent urinary tract infection and calculus irritation of the bladder mucosa. These symptoms are the main complaint of our patient while total hematuria was the reason for her presentation.
Pelvic ultrasonography and plain X-ray are diagnostic of bladder stone and radio opaque foreign body, [16] both were carried out in this case [Figure 1]. She had the procedure of cystoscopy and cystolithotomy for complete removal of IUCD-calculus. She has been symptom free since surgery.
Several minimally invasive methods of retrieval of foreign body from the bladder have been documented with complete clearance of bladder of the foreign body. [9],[10],[11],[12],[13],[14],[15],[16],[17] The use of cystoscopy, percutaneous approach and combination of cystoscopy and laparoscopy with laser has been described with satisfactory results. [17] These minimally invasive methods are advised because of the obvious advantages over open surgery where possible. In this patient, open surgery was performed because of limitation of minimally invasive procedures in our facility.
Our patient had an eventful insertion of IUCD. She presented 24 h after the insertion to the fertility clinic because of lower abdominal pain, during this visit the string of the IUCD was not visualized or felt in the vagina. These findings constitute a missing IUCD, suppose to have been sought for and this was not carried out in our patient. A pelvic ultrasound would have shown that the IUCD was not in the uterine cavity, but in the urinary bladder. Early retrieval would have prevented the morbidity of a longstanding vesical foreign body and stone that our patient endured for 10 years.
| Conclusion | | |
In a patient carrying IUCD, lower abdominal discomfort and a missing IUCD string at vaginal examination should raise suspicion of intravesical migration of the device. This diagnosis can readily be confirmed by pelvic ultrasound. Immediate retrieval of the device from the urinary bladder is important and would go a long way in preventing the burden of bladder stone disease.
| References | | |
| 1. | Thiery M. Pioneers of the intrauterine device. Eur J Contracept Reprod Health Care 1997;2:15-23. 
[PUBMED] |
| 2. | Güvel S, Tekin MI, Kilinç F, Peskircioglu L, Ozkardeº H. Bladder stones around a migrated and missed intrauterine contraceptive device. Int J Urol 2001;8:78-9.
|
| 3. | Ozgür A, Siþmanoðlu A, Yazici C, Coþar E, Tezen D, Ilker Y. Intravesical stone formation on intrauterine contraceptive device. Int Urol Nephrol 2004;36:345-8.
|
| 4. | Caspi B, Rabinerson D, Appelman Z, Kaplan B. Penetration of the bladder by a perforating intrauterine contraceptive device: A sonographic diagnosis. Ultrasound Obstet Gynecol 1996;7:458-60.
[PUBMED] |
| 5. | Katara AN, Chandiramani VA, Pandya SM, Nair NS. Migration of intrauterine contraceptive device into the appendix. Indian J Surg 2004;66:179-80.
|
| 6. | Saha S, Mahapatara L, Kaur N, Shrivastava U, Gupta S. Vesical calculus resulting from forgotten intrauterine contraceptive device. Internet J Gynecol Obstet 2009;11. Available from: http://archive.ispub.com/journal/the-internet-journal-of-gynecology-and-obstetrics/volume-11-number-2/vesical-calculus-resulting-from-forgotten-intrauterine-contraceptive-device.html [Last assessed on 2012 Jul 15].
|
| 7. | Parra Muntaner L, Rivas Escudero JA, Gómez Cisneros S, Borrego Hernando J, García Alonso J. Bilateral obstructive uropathy secondary to encrusted cystitis. Report of a case. Arch Esp Urol 1996;49:870-2.
|
| 8. | Schwartz BF, Stoller ML. The vesical calculus. Urol Clin North Am 2000;27:333-46.
[PUBMED] |
| 9. | El-Hefnawy AS, El-Nahas AR, Osman Y, Bazeed MA. Urinary complications of migrated intrauterine contraceptive device. Int Urogynecol J Pelvic Floor Dysfunct 2008;19:241-5.
[PUBMED] |
| 10. | Demirci D, Ekmekçioðlu O, Demirtaº A, Gülmez I. Big bladder stones around an intravesical migrated intrauterine device. Int Urol Nephrol 2003;35:495-6.
|
| 11. | Rajaie Esfahani M, Abdar A. Unusual migration of intrauterine device into bladder and calculus formation. Urol J 2007;4:49-51.
[PUBMED] |
| 12. | Nouira Y, Rakrouki S, Gargouri M, Fitouri Z, Horchani A. Intravesical migration of an intrauterine contraceptive device complicated by bladder stone: A report of six cases. Int Urogynecol J Pelvic Floor Dysfunct 2007;18:575-8.
[PUBMED] |
| 13. | Zakin D. Perforation of the bladder by the intrauterine device. Obstet Gynecol Surv 1984;39:59-66.
[PUBMED] |
| 14. | Haouas N, Sahraoui W, Youssef A, Thabet I, Mosbah AT. Intravesical migration of intrauterine device resulting in stone formation. J Gynecol Obstet Biol Reprod (Paris) 2006;35:288-92.
[PUBMED] |
| 15. | Dede FS, Dilbaz B, Sahin D, Dilbaz S. Vesical calculus formation around a migrated copper-T 380-A. Eur J Contracept Reprod Health Care 2006;11:50-2.
[PUBMED] |
| 16. | Amin U, Mahmood R. An unusual vesical calculus. J Radiol Case Rep 2009;3:10-3.
[PUBMED] |
| 17. | Rafique M. Intravesical foreign bodies: Review and current management strategies. Urol J 2008;5:223-31.
[PUBMED] |
[Figure 1], [Figure 2]
|
















