|


 |
| CASE REPORT |
|
| Year : 2013 | Volume
: 5
| Issue : 1 | Page : 45-47 |
|
|
Non-operative management of gallbladder perforation after blunt abdominal trauma
Rohan Kumar
Department of General Surgery, East Kent University NHS Foundation Trust, Ashford, Kent, TN24 0LZ, United Kingdom
| Date of Web Publication | 21-Sep-2013 |
Correspondence Address:
Rohan Kumar
Department of General Surgery, East Kent University NHS Foundation Trust, Ashford, Kent, TN24 0LZ
United Kingdom
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.118629

 Abstract Abstract | | |
Isolated gallbladder perforations following blunt abdominal trauma are very rare. They often present with insidious onset of symptoms a few days after the initial insult and an operative course of management ensues. This is in the form of a cholecystectomy and peritoneal lavage; more often via laparotomy rather than laparoscopically. Conservative management, in the form of cholecystostomy, percutaneous intraperitoneal drainage or cholecystorraphy has been described; however, these cases have invariably resulted in cholecystectomy eventually. The case uniquely highlights the successful non-operative management of isolated traumatic gallbladder perforation. Keywords: Cholecystectomy, cholecystorraphy, damage control surgery, endoscopic management
How to cite this article:
Kumar R. Non-operative management of gallbladder perforation after blunt abdominal trauma. J Surg Tech Case Report 2013;5:45-7 |
How to cite this URL:
Kumar R. Non-operative management of gallbladder perforation after blunt abdominal trauma. J Surg Tech Case Report [serial online] 2013 [cited 2016 May 25];5:45-7. Available from: http://www.jstcr.org/text.asp?2013/5/1/45/118629 |
| Introduction | |  |
Isolated gallbladder perforations following blunt abdominal trauma are very rare.
This case uniquely highlights the successful non-operative management of isolated traumatic gallbladder perforation in a patient that was considered to be a high risk operative candidate.
We employed successful non-operative management. Conservative management of this type of injury has not been previously reported.
| Case Report | | |
A 64-year-old man with a background of alcoholic liver disease presented to our Emergency Department following high velocity blunt abdominal trauma. He had been driving at 60 miles/h when he lost control and car rolled-over. He was seat-belt restrained and collision air bags were deployed. He managed to self-extricated on scene. Initial management and resuscitation was in accordance with Advanced Trauma Life Support® principles.
Admission Computed tomography (CT) scans were reported as unremarkable. He was admitted under cardiology for further management of a fast narrow complex tachycardia, atrial fibrillation as this was the only outstanding issue. A transthoracic echocardiogram 2 days later revealed a right ventricular thrombus and he was therefore commenced on therapeutic low molecular weight heparin.
On day eight post-trauma, this gentleman was referred to General Surgeons for abdominal distension and mild pain. He was stable hemodynamically and clinically he was found to have a soft, distended abdomen, with localized upper peritonism. A repeat CT scan reported free fluid and a perforated gallbladder [Figure 1].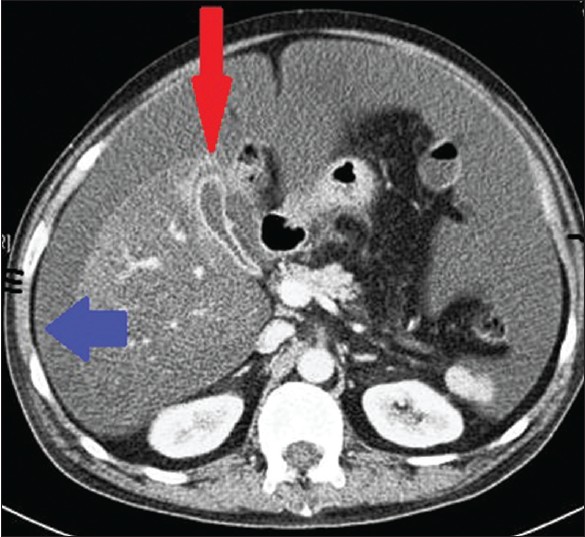 | Figure 1: Computed tomography showing gallbladder fundus perforation (red arrow) and free intraperitoneal fluid (blue arrow)
Click here to view |
In view of his comorbidities, the patient was considered high risk for a general anesthetic and major abdominal surgery. After multidisciplinary discussion conservative management was agreed. An endoscopic retrograde cholangio-pancreatogram (ERCP) with stent insertion was performed and a radiologically-guided intra-peritoneal drain inserted. A diagnosis of perforated gallbladder fundus was confirmed at ERCP [Figure 2]. Intravenous antibiotics were commenced.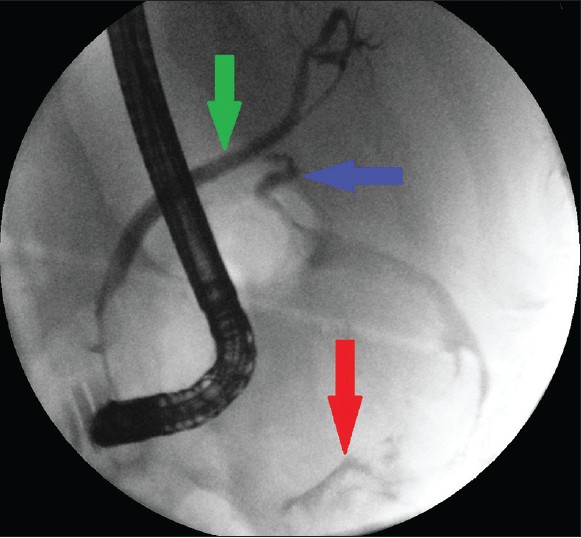 | Figure 2: Endoscopic retrograde cholangio‑pancreatogram showing common bile duct (green arrow), cystic duct (blue arrow) and extravasation of contrast from perforated gallbladder (red arrow)
Click here to view |
Over the next few days, the patient's condition improved. The intra-peritoneal drain was removed at day 12 post ERCP and the patient was discharged, uneventfully 35 days after the injury.
A follow-up ERCP 2 month later revealed a normal cholangiogram with no obvious leak and no filling defects. Stents were removed and sphincterotomy performed.
He was reviewed at 3 months and was doing well. Magnetic resonance cholangio-pancreatogram at 12 months showed no evidence of abnormality.
| Discussion | | |
Gallbladder injury secondary to blunt abdominal trauma is very rare, approximating 2% in the literature. [1],[2] The incidence of isolated gallbladder injury is even less as it tends to be protected anatomically by the liver, intestines, omentum, and rib cage. [3],[4] Pre-disposing risk factors include recent alcohol consumption, a distended post-prandial gallbladder with a thin wall and malposition. [1],[5] Traumatic gallbladder injuries usually present in three ways; as an additional finding during the damage control surgery (emergency laparotomy), with insidious onset of symptoms and signs a few days after the trauma and occasionally, a few weeks later with on-going non-specific abdominal complaints. [1],[5],[6]
Three classifications of gallbladder injury are reported. Laceration or perforation, which usually affect the gallbladder fundus, partial avulsions from the gallbladder fossa to near total traumatic cholecystectomy with or without disruption to the cystic duct and or cystic artery, and finally, contusions with an intramural hematoma contributing to wall necrosis and delayed perforation. Losanoff and Kjossev [7] have formally previously categorized injuries to the gallbladder in an attempt to guide operative intervention and there is an evidence to suggest that this classification system has merit in dictating management. [7]
Conservative measures such as cholecystostomy, percutaneous radiological intraperitoneal drainage or even cholecystorraphy have been reported, but found to be unsuccessful in the definitive control of gallbladder injury and invariably a cholecystectomy is required. [8] Others recommended an approach of diagnostic laparoscopy in equivocal trauma cases to identify gallbladder injury and once confirmed, proceed to laparoscopic cholecystectomy. [9],[10] Furthermore, operative management is recommended in gallbladder injuries associated with additional varying degrees of extra-hepatic biliary ductal injuries; either primary repair or duct to jejunum anastomosis with Roux-en-Y reconstruction. [3],[4]
Our patient was considered to be a high risk candidate for operation and we had to employ non-operative management, which was successful. Conservative management of this type of injury has not been previously reported.
| References | | |
| 1. | Liess BD, Awad ZT, Eubanks WS. Laparoscopic cholecystectomy for isolated traumatic rupture of the gallbladder following blunt abdominal injury. J Laparoendosc Adv Surg Tech A 2006;16:623-5. 
[PUBMED] |
| 2. | Carrillo EH, Lottenberg L, Saridakis A. Blunt traumatic injury of the gallbladder. J Trauma 2004;57:408-9.
[PUBMED] |
| 3. | Soderstrom CA, Maekawa K, DuPriest RW Jr, Cowley RA. Gallbladder injuries resulting from blunt abdominal trauma: An experience and review. Ann Surg 1981;193:60-6.
[PUBMED] |
| 4. | Sharma O. Blunt gallbladder injuries: Presentation of twenty-two cases with review of the literature. J Trauma 1995;39:576-80.
[PUBMED] |
| 5. | Bainbridge J, Shaaban H, Kenefick N, Armstrong CP. Delayed presentation of an isolated gallbladder rupture following blunt abdominal trauma: A case report. J Med Case Rep 2007;1:52.
[PUBMED] |
| 6. | Shirai Y, Yamazaki H, Tsukada K, Ohtani T, Muto T, Hatakeyama K. Stricture of the bile duct after blunt abdominal injury: Report of a case successfully managed by percutaneous biliary drainage. Eur J Surg 1994;160:515-8.
[PUBMED] |
| 7. | Losanoff JE, Kjossev KT. Complete traumatic avulsion of the gallbladder. Injury 1999;30:365-8.
[PUBMED] |
| 8. | Jaggard MK, Johal NS, Choudhry M. Blunt abdominal trauma resulting in gallbladder injury: A review with emphasis on pediatrics. J Trauma 2011;70:1005-10.
[PUBMED] |
| 9. | Pavlidis TE, Lalountas MA, Psarras K, Symeonidis NG, Tsitlakidis A, Pavlidis ET, et al. Isolated complete avulsion of the gallbladder (near traumatic cholecystectomy): A case report and review of the literature. J Med Case Rep 2011;5:392.
[PUBMED] |
| 10. | Contini S, Rubini P. Gallbladder injury in blunt abdominal trauma. Surg Endosc 2001;15:757.
[PUBMED] |
[Figure 1], [Figure 2]
|
















