|


 |
| CASE REPORT |
|
| Year : 2013 | Volume
: 5
| Issue : 2 | Page : 99-102 |
|
|
Successful laparoscopic removal of an ingested toothbrush
Karim Jamal1, Shalin Shaunak2, Sarandeep Kalsi3, Dhiren Nehra4
1 Departments of General Surgery SpR in Upper GI Surgery, Epsom and St. Helier University Hospitals NHS Trust, United Kingdom
2 CT1 in Surgery, Epsom and St. Helier University Hospitals NHS Trust, United Kingdom
3 Foundation Year 1 Doctor, Epsom and St. Helier University Hospitals NHS Trust, United Kingdom
4 Consultant in Upper GI Surgery, Epsom and St. Helier University Hospitals NHS Trust, United Kingdom
| Date of Web Publication | 13-Mar-2014 |
Correspondence Address:
Shalin Shaunak
10 Vincent Road, Isleworth, Middlesex, TW7 4LT
United Kingdom
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.128751

 Abstract Abstract | | |
Most ingested foreign bodies will pass through the gastrointestinal tract without any problems. On the other hand long, slender objects such as a toothbrush will rarely be able to negotiate the angulated and fixed retroperitoneal duodenal loop. Spontaneous toothbrush passage has never been described and therefore endoscopic or surgical removal is always required. Here we describe an asymptomatic young female presenting to out-patient clinic with a history of unintentional toothbrush ingestion 4 years prior. Endoscopic removal was unsuccessful because the toothbrush was partially embedded in to the gastric mucosa. We describe the second case to date of laparoscopic removal of a toothbrush via a gastrotomy with subsequent intra-corporeal repair of the defect. Keywords: Foreign body, gastronintestinal, laparoscopic, surgery, toothbrush
How to cite this article:
Jamal K, Shaunak S, Kalsi S, Nehra D. Successful laparoscopic removal of an ingested toothbrush. J Surg Tech Case Report 2013;5:99-102 |
How to cite this URL:
Jamal K, Shaunak S, Kalsi S, Nehra D. Successful laparoscopic removal of an ingested toothbrush. J Surg Tech Case Report [serial online] 2013 [cited 2016 May 25];5:99-102. Available from: http://www.jstcr.org/text.asp?2013/5/2/99/128751 |
| Introduction | |  |
Most ingested foreign bodies will pass through the gastrointestinal tract without any problems. On the other hand long, slender objects such as a toothbrush will rarely be able to negotiate the angulated and fi xed retroperitoneal duodenal loop. Spontaneous toothbrush passage has never been described and therefore endoscopic or surgical removal is always required. Here we describe an asymptomatic young female presenting to out-patient clinic with a history of unintentional toothbrush ingestion 4 years prior.
| Case Report | | |
We describe a case report of an 18-year-old girl who had accidentally swallowed a toothbrush. Immediately following the ingestion she attended accident and emergency but was discharged home as no foreign body was visible on an abdominal plain film. Four years later she presented to our surgical out-patient clinic with vague epigastric pain, adamant that she had previously ingested a toothbrush. Ultrasound and abdominal plain films confirmed a foreign body within the stomach. Endoscopic removal was then attempted on two separate occasions but the toothbrush was found to be straddling the pylorus and partial embedded within the gastric mucosa. Therefore, despite using a polypectomy snare and biopsy forceps, the toothbrush could not be safely freed. Endoscopic mucosectomy was not considered in this particular case because the toothbrush was deeply embedded.
The decision was taken to perform laparoscopic removal of the toothbrush. The patient was positioned in the supine position with sacrum at the edge of the table and the legs abducted in stirrups. The patient was given 1.2 g of augmentin intravenously as antibiotic prophylaxis. The surgeon stood in between the patient's legs with the assistant on the right hand side of the patient. A Veress needle was used to establish pneumoperitoneum with a working pressure of 12 mmHg and an initial 10-mm trocar was placed supra-umbilically as the camera port. Two further 5-mm trocars were placed under direct vision in the right and left subcostal margins both in the mid-clavicular line. A Nathanson liver retractor was introduced through a 5-mm epigastric incision to allow retraction of the left lobe of the liver. With a 10-mm 30-degree laparoscope and a reverse Trendelenburg position, the outline of the toothbrush could be clearly seen projecting on to the anterior gastric wall and extending in to the duodenum [Figure 1].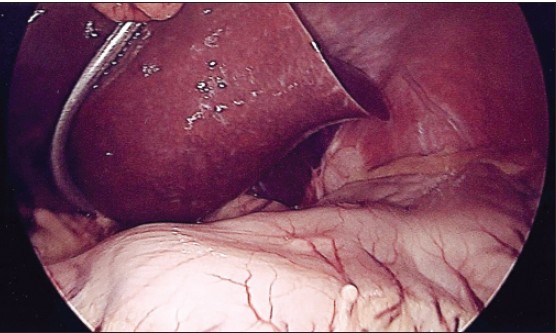 | Figure 1: Intraoperative image: Outline of the toothbrush visible on the anterior gastric wall
Click here to view |
Using hook diathermy, a 4-cm gastrotomy was made in the distal anterior gastric wall overlying the toothbrush. With the aid of two graspers we were able to manipulate and gently free the partially embedded toothbrush and allow safe removal from the stomach in its entirety [Figure 2].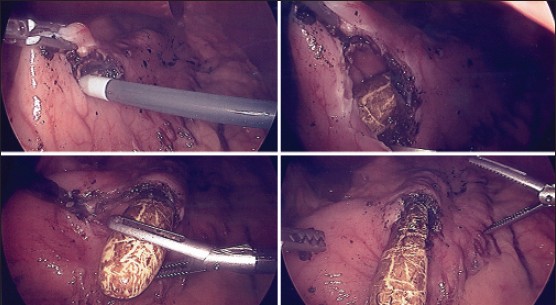 | Figure 2: Intraoperative image: Creation of gastrotomy with visualisation, instrumentation and subsequent mobilisation of retained toothbrush
Click here to view |
An endoloop was placed around the handle of the toothbrush with the string left long. A 5-mm 0-degree laparoscope was inserted down the right lateral 5-mm port allowing the string to be delivered via the 10-mm supraumbilical port. Subsequent manipulation of the string then facilitated delivery of the handle of the toothbrush in to the port. We then removed the 10-mm port from the abdomen thus allowing the toothbrush to be retrieved through the existing incision. The 10-mm port was re-introduced and the gastrostomy was laparoscopically sutured using a continuous 2-layer intracorporeal technique with ethibond 1/0 [Figure 3].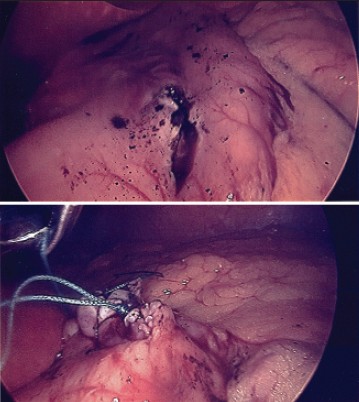 | Figure 3: Intraoperative image: Closure of gastrotomy wound using a continuous 2-layer intracorporeal technique
Click here to view |
We did not feel that an abdominal drain or nasogastric tube were required at the end of the procedure. The total operating time was 90 minutes and the patient was given a light diet the following day. After 48 hours, the patient was discharged as she was tolerating a normal diet, was pain free, and fully mobile. The patient was followed up in the surgical out-patient clinic 6 weeks after the operation and had made a full recovery.
| Discussion | | |
A multitude of factors are associated with the ingestion of foreign bodies. In children, it is often unintentional, occurring with a peak incidence of 6 months to 3 years. [1] In adults, it occurs in those with psychiatric disorders, developmental delay, drug intoxication and incarcerated individuals seeking secondary gain via release to a medical facility. [2] Edentulous individuals are at an increased risk of ingesting an obstructing food bolus or their dental prosthesis (3). Toothbrush ingestion most typically affects young females with an age range of 15-23 years old and with a significant incidence of psychiatric problems including bulimia or schizhophrenia. [3] Food bolus impaction is often secondary to underlying oesophageal pathology, such as eosinophilic oesophagitis. [4]
The decision as to whether an ingested foreign body requires removal and if so, the most appropriate timing of the procedure, is dependent on multiple factors. These include: The nature of the ingested object, patient age, time since ingestion, clinical condition of the patient, and dimensions and anatomical location of the ingested object. In general oesophageal foreign bodies and food impactions should be removed within 24 hours as delay beyond this leads to an increased risk of perforation. [5]
Special consideration should be given to disc or button battery ingestions which can rapidly lead to liquefactive necrosis and perforation: These should undergo urgent endoscopic removal. Other indications for emergency endoscopy include those with complete oesophageal obstruction i.e., those unable to tolerate secretions and the presence of sharp or pointed objects within the oesophageal lumen.
Approximately 80-90% of gastric foreign bodies will pass spontaneously through the gastrointestinal tract. [6] However, objects longer than 6 cm or wider than 2.5 cm will have difficultly negotiating the duodenal c-loop due to its fixed retroperitoneal position. [7] Therefore, these objects need removal to prevent complications such as perforation, obstruction, ulceration, haemorrhage, or fistula formation. [8] Although many sharp-pointed objects may pass spontaneously from the stomach, they should also be endoscopically retrieved to avoid distal complications. [9] In cases where sharp objects have migrated beyond endoscopic reach they should be followed radiographically to monitor their passage. Indications for surgical intervention include failure to progress after 72 hours, signs of abdominal sepsis or gastrointestinal haemorrhage. [10]
Most ingested foreign bodies can be removed endoscopically with a success rate of approximately 95%. [11] A wide variety of retrieval devices are available including forceps, snares, baskets, and nets. Practicing manipulation of a similar object can help the endoscopist to select the appropriate device. Although overtubes are associated with a small risk of perforation, some authors advocate their use to reduce the risk of aspiration and oesophagopharyngeal trauma. [12]
In an initial review of 31 cases of toothbrush ingestion and more recently 40 cases, [6] there were no instances of spontaneous passage with a number of complications described including pressure necrosis and perforation. [13] There is only case to date of a toothbrush leaving the upper gastrointestinal tract. [14] A schizophrenic patient ingested a toothbrush which managed to get through to the colon and present a year later with abdominal sepsis. At laparotomy a fistula was found between the hepatic flexure of the colon and the liver with an intervening abscess. This was dealt with by washout, wedge resection of the colon, removal of the toothbrush and closure of the colonic defect.
Ertan et al. reported the first successful endoscopic removal of a toothbrush in 1983 [15] with other case reports following on from this. [16] Equally, however, there have been a number of failed endoscopic removals described, [17],[18] including one that resulted in iatrogenic oesophageal perforation. [19] The geometric shape of a toothbrush can make it difficult to orientate the long axis with the gastroesophageal junction. In our particular case, the extremely delayed presentation had allowed the toothbrush to become partially embedded in the stomach and likely accounted for the failed endoscopic retrievals.
In the rare cases where endoscopic retrieval of a foreign body is unsuccessful or complications have developed such as perforation or obstruction surgical methods need to be employed. Laparotomy has traditionally been employed although there are a number of cases of laparoscopic removal of foreign bodies from the stomach. [20],[21] The advantages of laparoscopic removal are shorter hospital stay, reduced post-operative pain and reduced convalescence. [22] Laparotomy has been performed for failed endoscopic toothbrush removal. [23] We were able to identify only one case of a laparoscopic assisted removal of a toothbrush after failed endoscopic management. [24]
| Conclusions | | |
An ingested toothbrush will not pass spontaneously and has a significant risk of causing pressure necrosis or perforation which can result in life-threatening abdominal sepsis. As such, unlike smaller foreign bodies within the stomach, a trial of conservative therapy should not be employed. The best course of action is early endoscopy by a skilled operator. If this is unsuccessful either laparotomy or laparoscopy can be performed depending on local expertise.
| References | | |
| 1. | Cheng W, Tam PK. Foreign body ingestion in children: Experience with 1265 cases. J Pediatr Surg 1999;34:1472-6. 
|
| 2. | Palta R, Sahota A, Bemarki A, Salama P, Simpson N, Laine L. Foreign body ingestion: Characteristics and outcomes in a lower socieconomic population with predominantly intentional ingestion. Gastrointest Endosc 2009;69:426-33.
|
| 3. | Abdullah BJ, Teong LK, Mahadevan J, Jalaludin A. Dental prosthesis ingested and impacted in the oesophagus and orolaryngopharynx. J Otolaryngol 1998;27:190-4.
|
| 4. | Loh KS, Tan LK, Smith JD, Yeoh KH, Dong F. Complications of foreign bodies in the oesophagus. Otolaryngol Head Neck Surg 2000;123:613-6.
|
| 5. | Gordon AC, Gough MH. Oesophageal perforation after button battery ingestion. Ann R Coll Surg Engl 1993;75:362-4.
|
| 6. | Faust J, Schreiner O. A swallowed toothbrush. Lancet 2001;357:1012
|
| 7. | Ginsberg GG. Management of ingested foreign objects and food bolus impactions. Gastrointest Endosc 1995;41:33-8.
|
| 8. | Kirk AD, Bowers BA, Moylan JA, Meyers WC. Toothbrush swallowing. Arch Surg 1988;123:382-4.
|
| 9. | Carp L. Foreign bodies in the intestine. Ann J Surg 1927;85:575-91.
|
| 10. | Webb WA. Management of foreign bodies of the upper intestinal tract: Update. Gastrointest Endosc 1995;41:39-51.
|
| 11. | Li ZS, Sun ZX, Zou DW, Xu GM, Wu RP, Liao Z. Endoscopic management of foreign bodies in the upper GI tract: Experience with 1088 cases in China. Gastrointest Endosc 2006;64:485-92.
|
| 12. | Garrido J, Barkin JS. Endoscopic modification for safe foreign body removal. Am J Gastroenterol 1985;80:957-8.
|
| 13. | Chao HH, Chao TC. Perforation of the duodenum by an ingested toothbrush. World J Gastroenterol 2008;14:4410-2.
|
| 14. | Kim IH, Kim HC, Koh KH, Kim SH, Kim SW, Lee SO, et al. Journey of a swallowed toothbrush to the colon. Korean J Intern Med 2007;22:106-8.
|
| 15. | Ertan A, Kedia SM, Agrawal NM, Akdamar K. Endoscopic removal of a toothbrush. Gastrointest Endosc 1983;29:144-5.
|
| 16. | Chinitz MA, Bertrand G. Endoscopic removal of toothbrushes. Gastrointest Endosc 1990;36:527-30.
|
| 17. | Conway WC, Sugawa C, Ono H, Lucas CE. Upper GI foreign body: An adult urban emergency hospital experience. Surg Endosc 2007;21:455-60.
|
| 18. | Weiland ST, Schurr MJ. Conservative management of ingested foreign bodies. J Gastrointest Surg 2002;6:496-500.
|
| 19. | Selivanov V, Sheldon GF, Cello JP, Crass RA. Management of foreign body ingestion. Ann Surg 1984;199:187-91.
|
| 20. | Vishwaynath G. Laparoscopic removal of large sharp foreign bodies from the stomach. Oman Med J 2008;23:42-5.
|
| 21. | Karcz WK, Kulemann B, Seifert GJ, Schrag HJ, Küsters S, Marjanovic G, et al. Video. Laparoscopic extirpation of a fork from the duodenum. Surg Endosc 2011;25:2363.
|
| 22. | Schenk C, Mugomba G, Dabidian RA, Scheuerecker H, Glaser F. Laparoscopic extraction of a swallowed fork in a patient first diagnosed with bulimia nervosa. Surg Endosc 2002;16:361.
|
| 23. | Ayantunde AA, Oke T. A review of gastrointestinal foreign bodies. Int J Clin Pract 2006;60:735-9.
|
| 24. | Wishner JD, Rogers AM. Laparoscopic removal of a swallowed toothbrush. Surg Endosc 1997;11:472-3.
|
[Figure 1], [Figure 2], [Figure 3]
|
















