|


 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 7
| Issue : 1 | Page : 14-16 |
|
|
Female urethral anomalies in pediatric age group: Uncovered
Nikhil A Patil, Siddangouda B Patil, Vinay S Kundargi, Ashok N Biradar
Department of Urology, Shri B. M. Patil Medical College and Research Centre, Bijapur, Karnataka, India
| Date of Web Publication | 29-Jun-2016 |
Correspondence Address:
Siddangouda B Patil
Department of Urology, Shri B. M. Patil Medical College, Bijapur, Karnataka
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2006-8808.184937

 Abstract Abstract | | |
Female urethral anomalies such as epispadias and hypospadias have been rarely reported in the literature. Clinical diagnosis of female urethral anomalies is significant for management. Diagnosis may be missed leading to mismanagement of the clinical condition. Herein, we report a case of female epispadias and hypospadias managed by us at Tertiary Care Center. Keywords: Epispadias, female urethral anomalies, hypospadias
How to cite this article:
Patil NA, Patil SB, Kundargi VS, Biradar AN. Female urethral anomalies in pediatric age group: Uncovered. J Surg Tech Case Report 2015;7:14-6 |
How to cite this URL:
Patil NA, Patil SB, Kundargi VS, Biradar AN. Female urethral anomalies in pediatric age group: Uncovered. J Surg Tech Case Report [serial online] 2015 [cited 2018 Jul 1];7:14-6. Available from: http://www.jstcr.org/text.asp?2015/7/1/14/184937 |
| Introduction | |  |
Female epispadias is a rare congenital anomaly occurring in one in 484,000 female populations.[1] The patient presents with the characteristic appearance of external genitalia with or without urinary incontinence. Diagnosis can be missed may of the times. It is associated with the bifid clitoris. Female hypospadias is an infrequent birth deformity consisting in the fissure of the posterior (lower) wall of the urethra. Female hypospadias is characterized by shortening of the urethra and ectopia of the external urethral opening.
| Case Reports | | |
Case 1
A 5-year-old girl presented to us with complaints of urinary incontinence. History did not reveal any evidence of urinary tract infection, trauma or operative interventions. The child had normal developmental milestones. There were no other urological complaints. The child was voiding good quantity of urine. To quantify her incontinence it was around 4–5 pads/day. On examination of external genitalia revealed bifid clitoris [Figure 1]. Vagina and hymen were normal. The urethra was splayed and directed cranially with continuous dribbling of urine. Neurological examination was normal. Blood, urine routine and renal function tests were normal.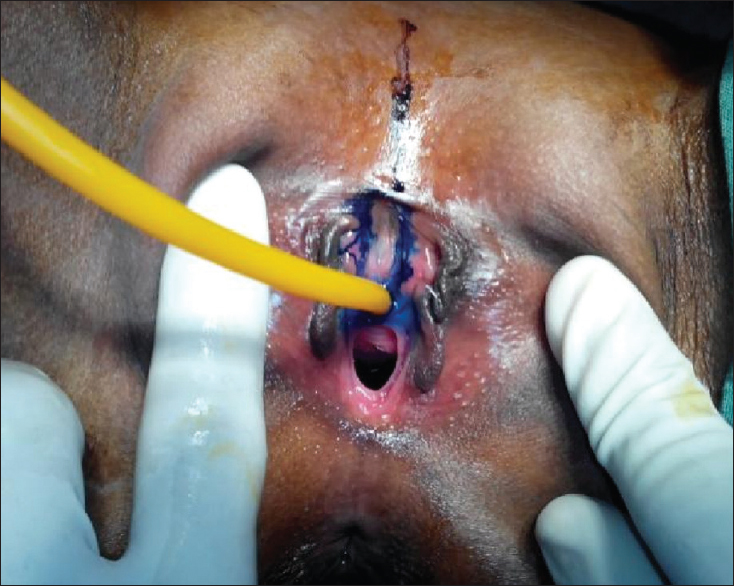 | Figure 1: Parallel incision taken for reconstruction of urethra. Note the bifid clitoris with deficient dorsal wall
Click here to view |
X-ray pelvis showed a defect in symphysis pubis [Figure 2]. Ultrasonography was done to rule out upper tract disease and was normal. Micturating voiding cystourethrogram revealed good capacity bladder. Cystourethroscopic assessment revealed normal appearing ureteric orifices and intact bladder neck.
A vertical parallel incision was taken along the urethra [Figure 1]. The urethra was mobilized to both the sides. Urethral reconstruction was done over a 10 French Foley's catheter. The redundant urethra was excised. The triangular area over the bifid clitoris was marked, and the raw area was sutured to obliterate the dead space. Postoperative period was uneventful. The catheter was removed after 9 days. The child was continent and could void well with no complaints. Postoperative ultrasonography was done at 6 weeks and 12 weeks with bladder capacity of 140 ml and 160 ml, respectively.
Case 2
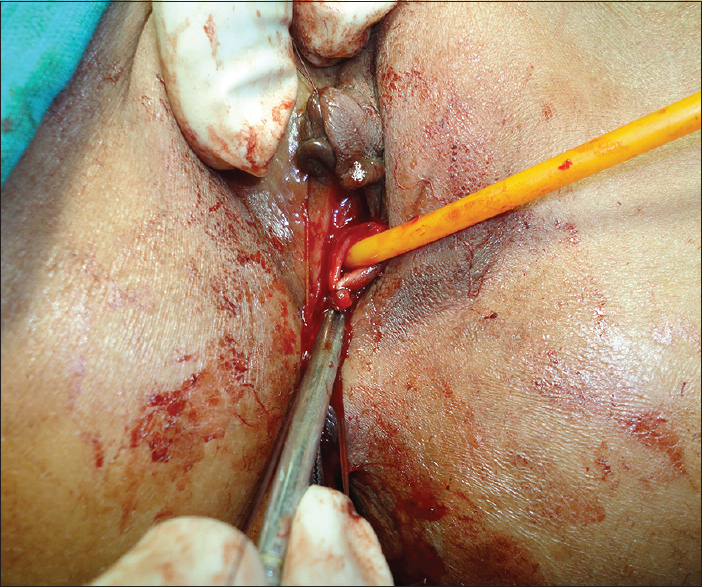
A 7-year-old girl presented to us with complaints of only true urinary incontinence. Her developmental milestones and higher motor functions were normal. There were no neurological deficits. Hemogram and urine routine was normal. On examination of external genitals, urethral meatus was caudally directed, and continuous leaking of urine was noted. The vagina was normal for the child's age on genitoscopy. Vulva and hymenal ring were normal. Cystourethrogram revealed short urethra. On cystourethroscopic assessment was done prior to a definitive procedure revealed short urethra (<1 cm). Urethral opening was seen almost close to the bladder neck. Both the ureteric orifices were normal, and bladder was normal with a capacity around 120 ml. There was no evidence of trabeculations. On insertion of 12 French Foleys catheter, the bulb of the catheter could be easily visualized [Figure 3]. The patient underwent primary urethral reconstruction over a 12 French Foleys catheter. The wide open urethral plate above the meatus and below the clitoral opening was mobilized by taking an inverted “U” incision [Figure 3]. After careful mobilization of the urethra, it was tabularized over 12 French Foleys catheter using absorbable suture [Figure 4]. The neometus formed after the reconstruction was sutured to the vagina after mobilization of the periurethral tissue. Catheter was kept for 11 days. The child was continent and voided adequate amount of urine with good flow. Postoperative ultrasonography was done at 12 weeks with bladder capacity of 220 ml. | Figure 3: Female hypospadias; inverted “U” incision is taken for reconstruction of urethra. Note: that the bulb of the catheter is visualized suggestive of short urethra
Click here to view |
| Disscussion | | |
Female urethral anomalies are rarely encountered in pediatric age group. These children present with a common symptom of true urinary incontinence. This poses a great challenge for pediatric urologists. We have presented both the forms of urethral anomalies that are epispadias and hypospadias.
Early diagnosis and early treatment play an important role to reduce the psychological and psychosocial problems and prevent urinary incontinence.[2] The importance of a careful examination should be emphasized, especially in female patients with chronic wetting of unknown cause. Davis has divided the female epispadias into three degrees: (1) Patulous urethra (milder form); (2) urethra dorsally split (intermediate degree) and; (3) cleft involving the whole urethra and bladder neck (severe degree).[3]
The genital defect is characterized by bifid clitoris and mons is depressed in shape and coated by a smooth area of skin. The vagina and the internal genetalia are normal. 30–75% of epispadias are associated with vesicoureteric reflux.[4] These children should undergo a complete radiological evaluation to identify and rule out other causes of incontinence. The role of the urodynamic study is indefinite but would help to justify the poor outlet resistance. Cystourethroscpy is required to access urethral length, bladder capacity and position of the ureteric orifice.
Female hypospadias is characterized by shortening of the urethra and ectopia of the external urethral opening. This deformity is rarely diagnosed because physicians are not well-informed about female hypospadias. There are various variants of female hypospadias.[5] These include:
- Low vaginal ectopia of the external urethral opening
- High vaginal ectopia of the external opening of the urethra
- Urovaginal (vesicovaginal) fusion of the neck of the urinary bladder with vagina accompanied with enuresis
- Urogenital sinus in females (ectopia of the external urethral opening in the urogenital sinus).
All the variants of female hypospadias must be surgically corrected as transposition of the external opening of the urethra from the vagina on the perineum under the clitoris in chronic urethritis. The second case mentioned above mimics sinus urogenitalis, but is not so because the majority of children born with a urogenital sinus have genital ambiguity.[6] At the same time, in the second case there was a healthy ventral urethral plate which is suggestive that it is a case of female hypospadias rather than sinus urogenitalis.
| Conclusion | | |
Diagnosis of female urethral anomalies and its treatment possess a great challenge to pediatric urologists. Careful clinical examination plays an important role in the diagnosis of these anomalies. The objectives of surgical repair include achievement of urinary continence with preservation of the upper urinary tracts and the reconstruction of functional and cosmetically acceptable genitalia.[7]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Singh DR, Sagade SN. Female epispadias. Indian J Urol 2000;16:163-4.   |
| 2. | Hendren WH. Congenital female epispadias with incontinence. J Urol 1981;125:558-64. |
| 3. | Gearhart JP, Mathews R. Exstrophy-epispadias complex. In: Wein AJ, editor. Campbell-Walsh Urology. 9 th ed. Philadelphia: Saunders; 2007. p. 3547-50. |
| 4. | Shetty MV, Bhaskaran A, Sen TK. Female epispadias. Afr J Paediatr Surg 2011;8:215-7. |
| 5. | Derevianko IM, Derevianko TI, Ryzhkov VV. Hypospadia in females. Urologiia 2007;78:26-8. |
| 6. | Rink RC, Kaefer M. Surgical management of disorders of sexual differentiation. Campbell and Walsh Urology. 10 th ed. Philadelphia: Elsevier Saunders; 2012. p. 3650. |
| 7. | Bhat AL, Bhat M, Sharma R, Saxena G. Single-stage perineal urethroplasty for continence in female epispadias: A preliminary report. Urology 2008;72:300-3. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|