|


 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 7
| Issue : 2 | Page : 29-31 |
|
|
Reduction and fixation of unstable fractures of the zygomatic arch: Report of a series of cases
Josuel Raimundo Cavalcante, Josuel Raimundo Cavalcante Junior, Tony Santos Peixoto, Talita Telles Pereira de Albuquerque, Alessandro Leite Cavalcanti
Department of Dentistry and Oral Maxillofacial Surgery, State University of Paraiba, Campina Grande, PB, Brazil
| Date of Web Publication | 6-Jul-2016 |
Correspondence Address:
Alessandro Leite Cavalcanti
School of Dentistry, State University of Paraiba, Baraunas Street, Bodocongo, Campina Grande, PB
Brazil
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2006-8808.185647

 Abstract Abstract | | |
Background: This study evaluated a series of cases of fracture in the zygomatic arch with displacement of the fractured segment. Materials and Methods: This prospective cohort study was conducted between May 2008 and February 2009. The study sample which consist of 10 patients of both genders with fractures in the zygomatic arch. The collection instrument included a specific sheet with data concerning the patient's age, cause, side of the fracture, type of treatment performed, recurrence and presence of lesions in the facial nerve. The radiographic indices of Waters and Hirtz were used. The data were presented by means of descriptive statistics (absolute and percentage distributions). Results: Most of the patients were male (90.0%), the most frequent etiology was a motorcycle accident (70.0%) and the left side was more affected (60.0%). There was no recurrence in any of the patients examined; however, 1 patient had a lesion in the facial nerve. The treatment performed for all patients was reduction and fixation with titanium miniplates. Conclusion: Fractures in the zygomatic arch are more frequent in young male individuals and the most common cause is a motorcycle accident, with the use of miniplates constituting an effective treatment without recurrence. Keywords: Accidents, facial injuries, maxillary fractures, traffic, zygomatic fractures
How to cite this article:
Cavalcante JR, Junior JR, Peixoto TS, de Albuquerque TT, Cavalcanti AL. Reduction and fixation of unstable fractures of the zygomatic arch: Report of a series of cases. J Surg Tech Case Report 2015;7:29-31 |
How to cite this URL:
Cavalcante JR, Junior JR, Peixoto TS, de Albuquerque TT, Cavalcanti AL. Reduction and fixation of unstable fractures of the zygomatic arch: Report of a series of cases. J Surg Tech Case Report [serial online] 2015 [cited 2018 Jul 1];7:29-31. Available from: http://www.jstcr.org/text.asp?2015/7/2/29/185647 |
| Introduction | |  |
Among the types of facial fractures, the zygomatic arch corresponds to the second most affected area, after the mandible. The posterior projection of the temporal process of the zygomatic bone, which presents a convex curve contour, is essential for this prevalence. [1]
Mandibular movements can be impaired by obstruction of the transit of the mandibular coronoid process by deformity of the zygomatic arch. Most of patients develop trismus; severe pain is not a frequent characteristic of the zygomatic arch trauma unless the fractured segment is movable. [2]
Radiographs in the occipitomental and submentovertex views are most commonly used for diagnosing fractures of the bone and zygomatic arch, depending on the location of the fracture points and degree of displacement. However, computed tomography is widely used, but it is not available at all institutions. [3]
Countless treatments for this type of pathology are described in the literature and the choice is mainly based on the type of fracture (whether it is stable or unstable). Therefore, a series of cases of fracture in the zygomatic arch with fractured segment displacement that were treated with stable internal fixation using plates and titanium screws were studied.
| Materials and methods | | |
This prospective cohort study was conducted between May 2008 and February 2009 in the city of Campina Grande, located in the countryside of the state of Paraíba 130 km from the state capital.
This study was conducted in compliance with the ethical guidelines issued by the resolution 196/96 of the Brazilian National Health Council/Ministry of health on research involving human subjects. The research project was independently reviewed and approved by the Ethics in Research Committee of the State University of Paraíba, Brazil.
The study population consisted of 10 patients who were recruited by means of a spontaneous referral by Hospital Antonio Targino, which is a reference center for urgent and emergency treatment of trauma victims. The inclusion criterion adopted was the presence of an isolated fracture in the zygomatic arch. Data were collected by a single researcher and registered in a specific sheet. The following variables were analyzed: Gender, cause of trauma, side of the fracture, type of treatment, recurrence and lesions in the facial nerve. The Waters and Hirtz radiographic indices were used, because both can confirm the presence of fractures in the zygomatic arch with displacement of the fractured segment.
The treatment for all patients was a reduction of the open area by a preauricular approach, with dilation of the skin in posteroanterior direction and a small incision over the zygomatic arch, enabling a good detachment of adjacent tissues; after the reduction, the rigid internal fixation was held with 2.0 mm straight miniplates and cortical screws (2 mm × 5 mm).
Data were organized with the aid of Epi-Info version 3.4 (Centers for Disease Control and Prevention, Atlanta, GA, USA). Descriptive statistics techniques were also used by means of absolute and percentage distributions.
| Results | | |
Most of the subjects were male (90%), with a mean age of 30.6 years and motorcycle accident was the major cause (70%). Regarding the side of the fracture, the left side was the most affected (60%). A lesion in the facial nerve was present owing to the type of wound in the case of only 1 patient; however, recurrence was not observed, as shown in [Table 1].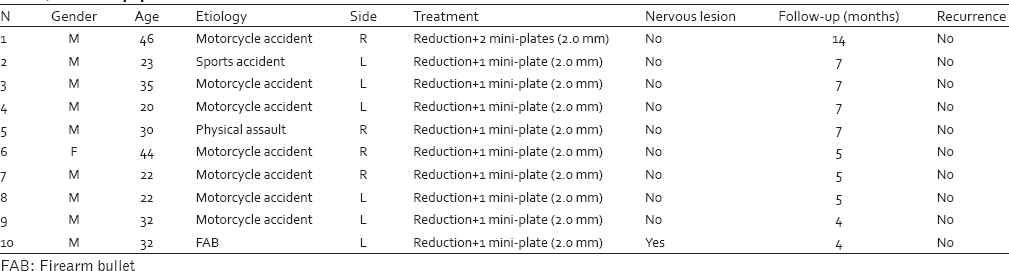 | Table 1: Patient distribution according to gender, age, etiology, affected side, treatment, presence of lesion in the nerve, follow-up period and recurrence
Click here to view |
| Discussion | | |
Fractures in the zygomatic complex represent a common facial trauma and the second or third most frequent fracture; this expressive occurrence is attributed to the prominent position of these bones in the facial skeleton. [4]
Alterations in the zygomatic arch conformation [2] and locking of movement of the mouth opening derived from obstruction in the course of the mandibular coronoid process by deformity of the arch and the resulting discomfort are common clinical findings in zygomatic arch fractures. [1],[2] Thus, the diagnosis of this condition is based on the patient's history and clinical examination and complemented by radiographic examination. [5]
Characteristics of the occurrence of these fractures, such as incidence, etiology, age and gender, vary mainly due to the socio-economic and educational conditions of the study population. [2],[4] A greater proportion of male patients was observed in this study, a finding also reported by other authors, with percentages of 83.6% [6] and 79.5% respectively. [7]
With regard to age group, most of the patients were between 20-year and 35-year-old, confirming the statement that young adults are most commonly affected, as previously described. [3],[6] The predominance of younger male patients is linked to the consumption of alcohol and participation in sports activities. [8]
Causes of the zygomatic arch fractures are varied, including physical assault, [4] car accidents, [3] falls [6] and work and sports accidents. [9] In the present work, among the 10 cases analyzed, 7 were consequences of motorcycle accidents, confirming the findings reported in the literature that highlight the wide use of this means of transportation regionally. [4] In this sense, some authors have already highlighted that in the city of Campina Grande, there is a large number of motorcycles, resulting in the city having one of the largest fleets of motor vehicles in the northeast countryside. [10]
Radiographs in the occipitomental view (or posteroanterior of waters) enable proper visualization of fractures in the zygomatic bone; those in the submentovertex view (or of Hirtz) are most frequently used for the diagnosis of the zygomatic arch fractures. [2],[11] The easy implementation and low cost of these radiographic indices facilitate the diagnosis and improve the treatment outcomes. [5],[11]
The treatment for zygomatic arch fractures aims to restore the facial contour and occlusion and mandibular movement, in addition to restoring facial sensitivity. These treatments can be performed through a transcutaneous approach in the face via Ginestet's technique, an intrabuccal approach via Keen's technique and a temporal transcutaneous approach via Gilles' technique, all which are widely employed when a line of fracture is present. [2]
When stability after closed reduction is not achieved, several apparatuses that do not require surgical approaches to be implemented can be used, such as Foley's catheter, inflated balloon, or cerclage of the zygomatic arch. [2] However, segmental stability is not ensured. To ensure reduction and stability of the fractured zygomatic arch segment, it is important to place the synthesis material; [12] particularly, in this series of cases, mini-plates and screws in the 2.0 system were used. The use of 2 screws per bone segment prevents the loss of stability, especially in support areas of stress in the maxillofacial region. [5]
When osteosynthesis is selected, a preauricular approach or an approach by extension of the infrapalpebral route is recommended. [12] Although permanent lesions of the facial nerve are reduced [13],[14] via this type of approach, with rates reported to a range from 9% to 18% in one study [15] and from 1.5% to 32% in another study, [16] lesions of the facial nerve resulting from the treatment were not observed in any of the patients in this series of cases, excluding the case of one patient in whom the lesion was caused by the trauma itself.
| Conclusion | | |
The use of miniplates and screws to treat unstable fractures of the zygomatic arch was demonstrated to be safe and effective without recurrence or lesions in the facial nerve in the patients examined.
| References | | |
| 1. | Gülicher D, Krimmel M, Reinert S. The role of intraoperative ultrasonography in zygomatic complex fracture repair. Int J Oral Maxillofac Surg 2006;35:224-30.  |
| 2. | Torres CS, Almeida DV, Neto NR, Oliveira MA, Sobrinho JB. Containment cerclage in fracture of the zygomatic arch: A case report. Rev Cir Traumatol Buco-Maxilo-fac 2008;8:29-34. |
| 3. | Sassi LM, Dissenha JL, Bezeruska C, Guebur MI, Hepp V, Radaelli RL, et al. Fractures of the zygomatic: Report of 50 cases. Rev Bras Cir Cabeça Pescoço 2009;38:246-7. |
| 4. | Peron MF, Ferreira GM, Camarini ET, Filho LI, Farah GJ, Pavan AJ. Epidemiological surveying of the fractures of the zigomatic complex in the residence service in surgery and bucomaxillofacial traumatology of UEM in the period of 2005-2006. Rev Odontol UNESP 2009;38:1-5. |
| 5. | Vier FV, Marinho SA, Gabriel JG, Costa NP, Veeck EB, Warszawsky D. Sequela after zygomatic fracture reduction using Kirschner wire: A case report. Radiol Bras 2005;38:157-60. |
| 6. | Gondola AO, Pereira Júnior ED, Pereira AM, Antunes AA. Zygomatic fractures epidemiology: A 10-year-analysis. J Dent Sci 2006;21:158-62. |
| 7. | Marques AC, Guedes LJ, Sizenando RP. Incidence and etiology of face fractures in the Venda Nova region-Belo Horizonte, MG-Brazil. Rev Med Minas Gerais 2010;20:500-2. |
| 8. | Bissada E, Chacra ZA, Ahmarani C, Poirier J, Rahal A. Orbitozygomatic complex fracture reduction under local anesthesia and light oral sedation. J Oral Maxillofac Surg 2008;66:1378-82. |
| 9. | Manganello-Souza LC, Barros JJ. Fraturas do complexo zigomático. In: Manganello-Souza LC, Barros JJ, editors. Traumatismo Bucomaxilofacial. São Paulo: Roca; 1993. p. 325-42. |
| 10. | Cavalcanti AL, Monteiro BV. Mortality by external causes in adults in the city of Campina Grande, Paraiba, Brazil. Sci Med 2008;18:160-5. |
| 11. | Shinohara EH, Junior JP. Simple fracture of zygomatic arcus-excusing protection pomp. Rev Assoc Paul Cir Dent 2000;55:259. |
| 12. | Ellis E 3 rd , el-Attar A, Moos KF. An analysis of 2,067 cases of zygomatico-orbital fracture. J Oral Maxillofac Surg 1985;43:417-28. |
| 13. | Weinberg S, Kryshtalskyj B. Facial nerve function following temporomandibular joint surgery using the preauricular approach. J Oral Maxillofac Surg 1992;50:1048-51. |
| 14. | do Egito Vasconcelos BC, Bessa-Nogueira RV, da Silva LC. Prospective study of facial nerve function after surgical procedures for the treatment of temporomandibular pathology. J Oral Maxillofac Surg 2007;65:972-8. |
| 15. | Hong Y, Gu X, Feng X, Wang Y. Modified coronoid process grafts combined with sagittal split osteotomy for treatment of bilateral temporomandibular joint ankylosis. J Oral Maxillofac Surg 2002;60:11-8. |
| 16. | Vasconcelos BC, Bessa-Nogueira RV, Cypriano RV. Treatment of temporomandibular joint ankylosis by gap arthroplasty. Med Oral Patol Oral Cir Bucal 2006;11:E66-9. |
[Table 1]
|















