|


 |
| SURGICAL DEBATE |
|
| Year : 2015 | Volume
: 7
| Issue : 2 | Page : 42-44 |
|
|
Anterior palatal island advancement flap for bone graft coverage: technical note
Amin Rahpeyma1, Saeedeh Khajehahmadi2
1 Associate Professor of Oral and Maxillofacial Surgery, Oral and Maxillofacial Diseases Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
2 Assistant Professor of Oral and Maxillofacial Pathology, Dental Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
| Date of Web Publication | 6-Jul-2016 |
Correspondence Address:
Saeedeh Khajehahmadi
Dental Research Center, Mashhad University of Medical Sciences, Vakilabad Boulevard, P.O. Box: 91735-984, Mashhad
Iran
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2006-8808.185655

 Abstract Abstract | | |
Background: The most important step in bone graft management is soft tissue coverage. Dehiscence of the wound leads to graft exposure and subsequent problems. Purpose: This study introduces an axial pattern flap for bone graft coverage in anterior maxilla. Patients and Methods: Use of Anterior Palatal Island Advancement Flap is presented by the authors. It is a mucoperiosteal flap with axial pattern blood supply, based on nasopalatine artery. It is easy to raise and predictable. Results: Anterior Palatal Island Advancement Flap was effective in bone graft coverage in premaxillary edentulous area. Conclusion: It can be used as an aid for bone graft coverage of premaxillary edentulous ridge, where the need for mucosa is small in width but long in length. Keywords: Anterior maxilla, bone graft, dental implant, palatal advancement flap
How to cite this article:
Rahpeyma A, Khajehahmadi S. Anterior palatal island advancement flap for bone graft coverage: technical note. J Surg Tech Case Report 2015;7:42-4 |
How to cite this URL:
Rahpeyma A, Khajehahmadi S. Anterior palatal island advancement flap for bone graft coverage: technical note. J Surg Tech Case Report [serial online] 2015 [cited 2018 Jul 1];7:42-4. Available from: http://www.jstcr.org/text.asp?2015/7/2/42/185655 |
| Introduction | |  |
The most important step in bone graft augmentation of alveolar process is soft tissue coverage. Dehiscence of the wound leads to graft exposure and subsequent problems. [1] When the graft is placed on the bone (onlay) or in between the split alveolar ridge (inlay), then the added width will prevent tensionless closure of the soft tissue.
There are several ways to overcome this problem including wide subperiosteal undermining, periosteal hatching, using tissue expanders before bone graft, and finally soft tissue flaps for bone graft coverage. [2],[3],[4],[5] In the anterior maxilla that is the most esthetic demand area in the mouth, restorative and prosthodontic treatments should have ideal characteristics, as well as possible. This paper reports an Anterior Palatal Island Advancement Flap for bone graft coverage in anterior maxilla.
| Patients and methods | | |
Patients
The patient was a 48-year-old female, who was referred for maxillary posterior segmental repositioning and mandibular subapical osteotomy to level the occlusal plane and provide sufficient space for dental prosthesis. Maxilla was edentulous in between the remaining canine root teeth; the prosthodontist's plan was to reconstruct the anterior maxilla with fixed dental implants and dowel-core crown of the canine teeth after crown lengthening. Cone-beam computed tomography of the maxillary anterior region showed thin remaining bone. The region needs to be augmented for hard tissue replacement. Wedge of the bone that was harvested from anterior mandibular subapical osteotomy was used for bone grafting [Figure 1].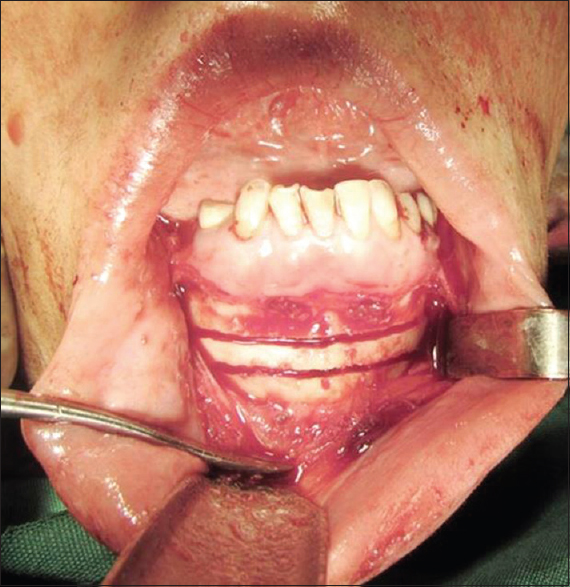 | Figure 1: Wedge of the bone was harvested from anterior mandibular subapical osteotomy
Click here to view |
The bone graft was covered by reflecting the labial mucoperiosteal flap and exposed bone in ridge crest was covered by Anterior Palatal Island Advancement Flap [Figure 2].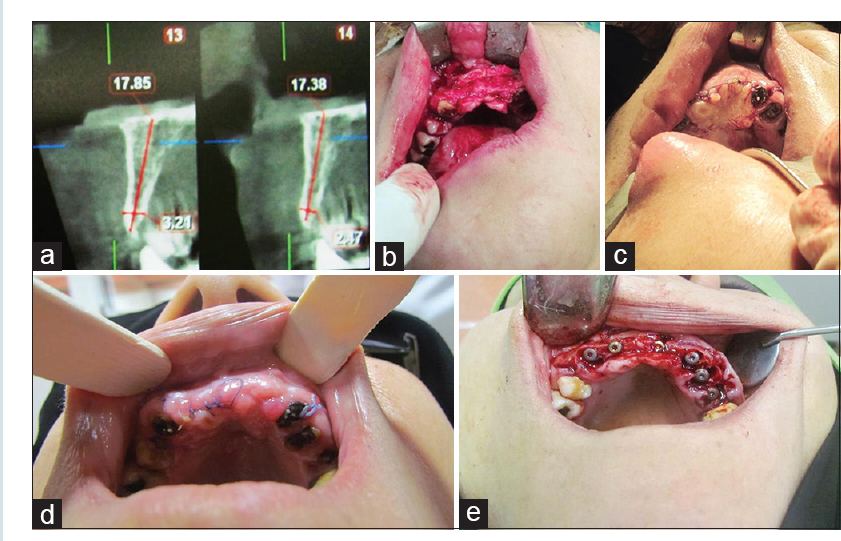 | Figure 2: (a) Cone-beam computed tomography of anterior maxilla with thin width alveolar ridge. (b) Maxillary anterior buccal onlay bone grafting. (c) Tensionless coverage of bone graft with Anterior Palatal Island Advancement Flap. (d) Postoperative photograph 3 weeks after operation. (e) Implant insertion into the bone graft and adjacent fresh extraction socket
Click here to view |
Methods
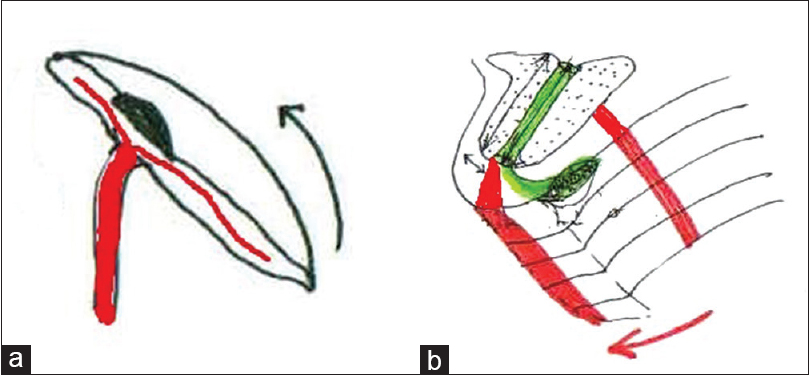
Two vertical palatal parallel-releasing incisions, mesial to the maxillary canines, were cut which are 2 cm in length. Full-thickness palatal mucoperiosteal flap was elevated from the bone with the aid of fine periosteal elevator using great care to avoid injury to the incisive foramen contents. After delicate flap elevation, the third horizontal incision in the palate connects the vertical cuts.
The only attachment of this flap is nasopalatin neurovascular bundle. The flap was advanced 2-3 mm and sutured to the labial flap. All incisions were sutured except the third palatal horizontal incision [Figure 3].
The bony gap behind it was let to be covered with granulation tissue and finally epithelialized.
| Results | | |
Anterior Palatal Island Advancement Flap was effective in bone graft coverage in premaxillary edentulous area [Figure 4].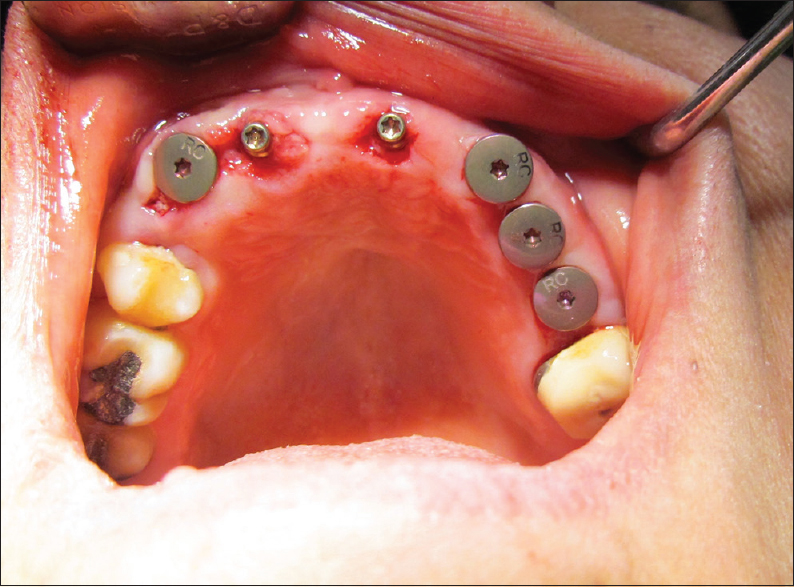 | Figure 4: Healing caps in position on implant body and ideal gingival relationship
Click here to view |
| Discussion | | |
When there is a need of soft tissue flaps in anterior maxilla for bone graft coverage, some limited choices are available. The transferred tissue in ideal conditions should have color and consistency similar to the adjacent tissues. Buccal mucosal transposition flaps (finger flaps) are not ideal because the transferred tissue is mobile and nonkeratinized. [6] Palatal flaps are available for providing anterior maxillary bone graft coverage for the mucosa. Flaps that formed from palatal mucosa for this purpose are rotated palatal flap and palatal advanced flap. [7],[8] Flaps from palatal subepithelial connective tissue (CT) are vascularized interpositional periosteal-CT, roll, modified roll, and vascularized periosteal membrane flaps. [9],[10],[11],[12]
Second group flaps need time for secondary epithelialization. Palatal mucosa is supplied by six pairs of arteries. [13] Posterior Palatal Island Flaps are nourished by greater palatine artery but anterior palatal island advancement flap is anteriorly based mucoperiosteal flap and relays on nasopalatine artery. It is indicated when the anterior maxillary incisors (four teeth) have been lost and there is a need for 2-3 mm advancement of palatal flap. It is anticipated that in older patients with enlarged nasopalatine canal, the amount of flap advancement will increase. [14]
This flap is recommended for bone graft coverage just in premaxillary edentulous space. In the situation that two central maxillary incisors are lost, flap elevation is difficult and if the edentulous span is long, then blood perfusion of the flap becomes compromised.
| Conclusion | | |
Anterior Palatal Island Advancement Flap is axial pattern and can be used as an aid for bone graft coverage of premaxillary edentulous space, where the need for mucosa is small in width but long in length.
Financial support and sponsorship
This study was supported by a grant (No:940684) from the Vice Chancellor of Research of Mashhad University of Medical Sciences for assessing reliability of Anterior Palatal Island Advancement Flap in animal study.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Chaushu G, Mardinger O, Peleg M, Ghelfan O, Nissan J. Analysis of complications following augmentation with cancellous block allografts. J Periodontol 2010;81:1759-64.  |
| 2. | Garg AK. Subnasal elevation and bone augmentation in dental implantology. Dent Implantol Update 2008;19:17-21. |
| 3. | Heller AL, Heller RL, Cook G, D′Orazio R, Rutkowski J. Soft tissue management techniques for implant dentistry: A clinical guide. J Oral Implantol 2000;26:91-103. |
| 4. | Abrahamsson P, Wälivaara DÅ, Isaksson S, Andersson G. Periosteal expansion before local bone reconstruction using a new technique for measuring soft tissue profile stability: A clinical study. J Oral Maxillofac Surg 2012;70:e521-30. |
| 5. | Nemcovsky CE, Moses O, Artzi Z, Gelernter I. Clinical coverage of dehiscence defects in immediate implant procedures: Three surgical modalities to achieve primary soft tissue closure. Int J Oral Maxillofac Implants 2000;15:843-52. |
| 6. | Rosenquist B. A comparison of various methods of soft tissue management following the immediate placement of implants into extraction sockets. Int J Oral Maxillofac Implants 1997;12:43-51. |
| 7. | Nemcovsky CE, Artzi Z, Moses O. Rotated palatal flap in immediate implant procedures. Clinical evaluation of 26 consecutive cases. Clin Oral Implants Res 2000;11:83-90. |
| 8. | Goldstein M, Boyan BD, Schwartz Z. The palatal advanced flap: A pedicle flap for primary coverage of immediately placed implants. Clin Oral Implants Res 2002;13:644-50. |
| 9. | Rahpeyma A, Khajeh Ahmadi S, Reza Hosseini V, Azimi H. A bilateral pediculated palatal periosteal connective tissue flap for coverage of large bone grafts in the anterior maxillary region. Iran J Otorhinolaryngol 2012;24:143-6. |
| 10. | Veisman H. "The palatal roll". Soft tissue ridge augmentation using a subepithelial connective tissue pedicle graft. Oral Health 1998;88:47, 49-51. |
| 11. | Scharf DR, Tarnow DP. Modified roll technique for localized alveolar ridge augmentation. Int J Periodontics Restorative Dent 1992;12:415-25. |
| 12. | Santana RB, de Mattos CM. Efficacy of vascularized periosteal membranes in providing soft tissue closure at grafted human maxillary extraction sites. Int J Oral Maxillofac Implants 2009;24:81-7. |
| 13. | Zhang KQ. Artery supply of the lip and palate in normal and cleft patients. Zhonghua Kou Qiang Yi Xue Za Zhi 1994;29:30-3, 63. |
| 14. | Mardinger O, Namani-Sadan N, Chaushu G, Schwartz-Arad D. Morphologic changes of the nasopalatine canal related to dental implantation: A radiologic study in different degrees of absorbed maxillae. J Periodontol 2008;79:1659-62. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|