|


 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 7
| Issue : 2 | Page : 45-47 |
|
|
Primary squamous cell carcinoma of stomach: A rare entity - case report and brief review of literature
Rashmi Patnayak1, Venkatarami Reddy2, Radhakrishnan2, Amitabh Jena3
1 Department of Pathology, Sri Venkateswara Institute of Medical Sciences, Tirupati, Andhra Pradesh, India
2 Department of Surgical Gastroenterology, Sri Venkateswara Institute of Medical Sciences, Tirupati, Andhra Pradesh, India
3 Department of Surgical Oncology, Sri Venkateswara Institute of Medical Sciences, Tirupati, Andhra Pradesh, India
| Date of Web Publication | 6-Jul-2016 |
Correspondence Address:
Rashmi Patnayak
Department of Pathology, Sri Venkateswara Institute of Medical Sciences, Tirupati - 517 507, Andhra Pradesh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2006-8808.185656

 Abstract Abstract | | |
Very few case reports of pure squamous cell carcinoma (SCC) of stomach are available in the world literature. The exact pathology of this uncommon carcinoma in stomach remains unknown. This is an additional case report of SCC in an elderly female arising in the gastric antrum. She underwent distal gastrectomy, gastrojejunostomy and jejunojejunostomy. The histopathology was reported as SCC of stomach without any adenocarcinomatous component. She had no other source of extra gastric primary SCC. After surgery, the patient was advised adjuvant chemotherapy. This is an additional case of primary SCC of stomach. Keywords: Primary, squamous cell carcinoma, stomach
How to cite this article:
Patnayak R, Reddy V, Radhakrishnan, Jena A. Primary squamous cell carcinoma of stomach: A rare entity - case report and brief review of literature. J Surg Tech Case Report 2015;7:45-7 |
How to cite this URL:
Patnayak R, Reddy V, Radhakrishnan, Jena A. Primary squamous cell carcinoma of stomach: A rare entity - case report and brief review of literature. J Surg Tech Case Report [serial online] 2015 [cited 2018 Jul 1];7:45-7. Available from: http://www.jstcr.org/text.asp?2015/7/2/45/185656 |
| Introduction | |  |
Primary squamous cell carcinoma (SCC) of stomach is extremely rare. [1] Very few cases of pure, primary SCC of the stomach are reported in world literature. Their number is approximately <100. [2] The exact pathogenesis of primary SCC is not known. [1] Various theories have been suggested to explain the occurrence of SCC in stomach.
| Case report | | |
An 80-year-old postmenopausal female presented with complaint of epigastric pain for 2 weeks. The pain was of burning type. It was not associated with vomiting, fever or jaundice. She also complained of loss of appetite and weight. She gave a history of on and off fever 2 months back, which was diagnosed as typhoid and she received treatment for the same. Per abdominal examination revealed a swelling of the size 4 cm × 5 cm in the right hypochondrium and epigastric region.
Her routine investigations were within normal limit. Ultrasonography examination revealed irregular hypo echoic wall thickening in the duodenum. Computed tomography scan of the abdomen revealed the evidence of concentric thickening of pylorus of the stomach.
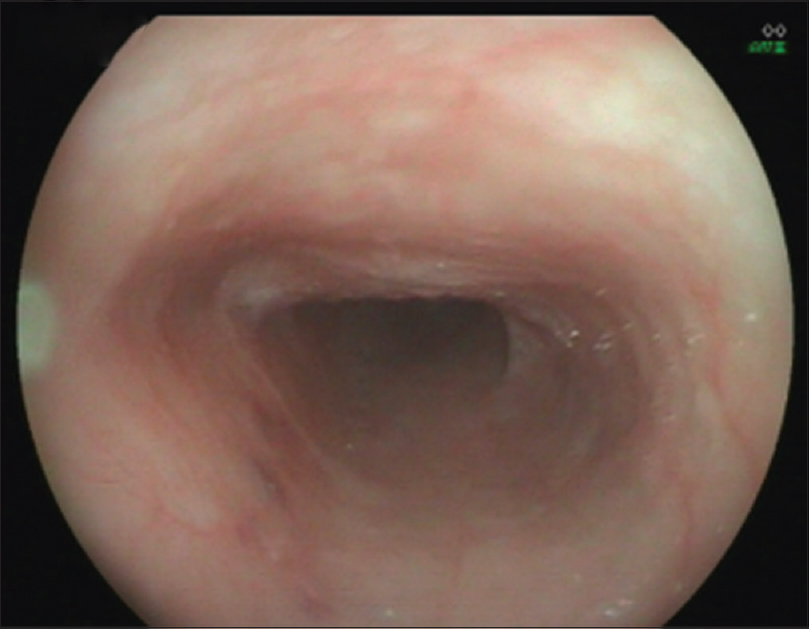
Endoscopy showed an ulcero-infiltrative growth in antrum extending onto the anterior wall of first part of duodenum [Figure 1]. It also revealed a normal esophagus [Figure 2]. Intra-operatively the tumor was present in the distal part of stomach. In the rest of the viscera no abnormality was noted.
Following this she underwent distal gastrectomy, gastrojejunostomy and jejunojejunostomy.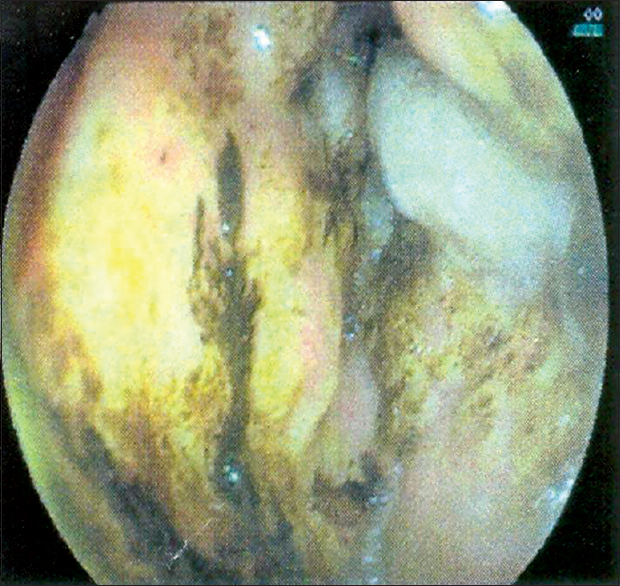 | Figure 1: Endoscopy showing an ulcero-infiltrative growth in antrum extending onto the anterior wall of first part of duodenum
Click here to view |
Gross examination of the distal gastrectomy specimen revealed an ulceroproliferative growth measuring 8 cm × 5 cm present in the antrum [Figure 3].
Histopathological examination of the distal gastrectomy specimen revealed the lesional component. The tumor comprised of polygonal cells with hyperchromatic nuclei and abundant amount of eosinophilic cytoplasm. Mitotic figures were frequently noted. The tumor cells were arranged in the form of sheets and nests. Individual cell keratinization and small areas of keratin formation is also noted. The tumor was seen infiltrating all the layers of the stomach. Multiple sections did not reveal any glandular component or mucin. Squamous metaplasia foci were also not seen. There was no evidence of Helicobacter, fungal, or parasitic infection [Figure 4] and [Figure 5]. | Figure 3: Distal gastrectomy specimen with an ulceroproliferative growth
Click here to view |
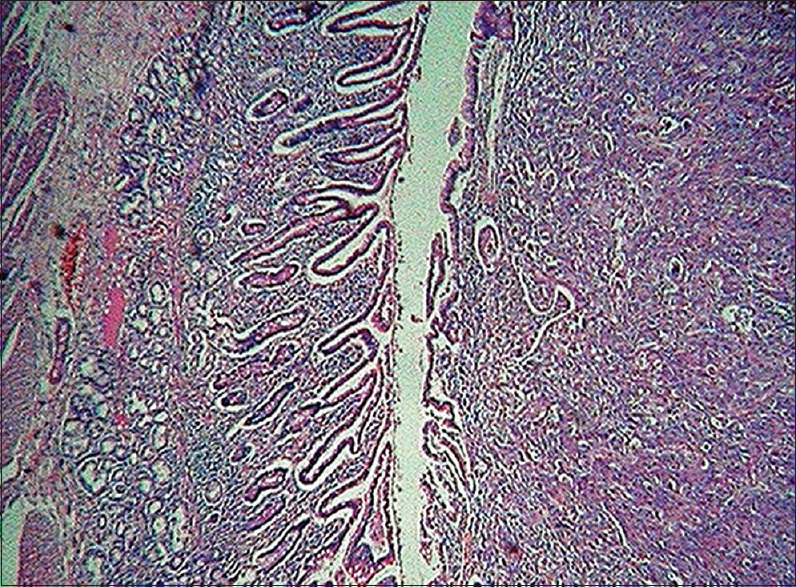 | Figure 4: Neoplastic squamous cells islands in antrum and duodenum (H and E, ×4)
Click here to view |
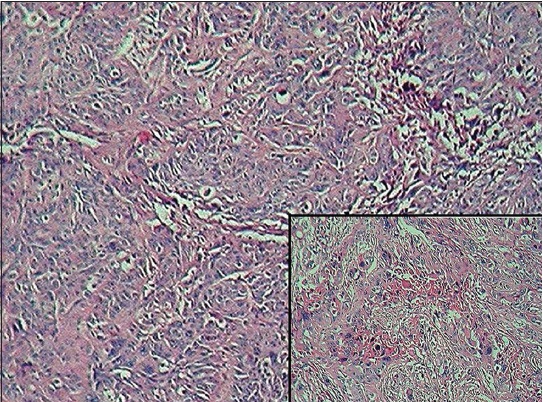 | Figure 5: Neoplastic squamous cells islands with pleomorphism (H and E, ×10) inset: Areas of keratin formation
Click here to view |
The proximal (gastric) and distal (duodenal) resected margins were free from involvement by tumor. The isolated perigastric lymph nodes were reactive in nature.
Her postup period was uneventful. Because of her old age and poor performance status, she was managed symptomatically. No other source of extra gastric primary SCC was noted. Adjuvant chemotherapy was advised, but the patient refused further treatment.
| Discussion | | |
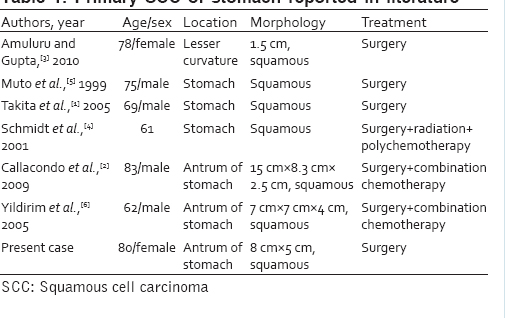
Pure SCC of the stomach is an extremely rare entity. Its worldwide incidence is around 0.04-0.07%. [3] Very few cases are reported in the world literature [Table 1]. These reports show a peak incidence in the sixth decade of life and male predominance. [4],[5],[6]
According to Parks for a diagnosis of primary SCC of the stomach the criteria required are absence of tumor in the cardia, no tumor extension to the esophagus and no evidence of SCC in any other part of the body. [7] The present case fulfilled the above mentioned criteria.
Boswell and Helwing opined that in histopathology of SCC of the stomach, keratinizing cell masses with pearl formation are typical. [8] In the present case also there were areas of keratin formation, squamous pearls and individual cell keratinization. According to them a mosaic pattern of cell arrangement with sharp borders, intercellular bridges and a high concentration of sulfhydryl or disulfide groups, indicating the presence of keratin, are characteristics of SCC of the stomach. [8]
The exact pathogenesis of primary SCC is not known. [1] Several theories have been proposed regarding the origin of pure SCC of the stomach. [3] They include the presence of totipotential (stem) cells, an area of ectopic squamous cell nests, squamous metaplasia of glandular epithelium secondary to chronic mucosal damage and squamous differentiation of preexisting adenocarcinoma. [3],[5],[6] One theory also suggests Epstein-Barr virus (EBV) infection, in the pathogenesis of SCC arising in the stomach. [1]
In the present case there were no foci of squamous metaplasia in the adjacent gastric mucosa. We have not done studies to detect the presence of EBV in our case.
Mori et al. in their study reexamined histopathological sections of three primary SCC of the stomach. They noted revealed minute areas of adenocarcinoma in addition to large areas of SCC. Hence, they opined that some gastric SCCs may be adenosquamous carcinomas with a predominant squamous component. [9]
In the present case, multiple sections did not reveal presence of any adenocarcinomatous component or mucin.
Due to the advanced stage at the time of diagnosis in most of these cases, the prognosis is generally poor. [4],[5],[6]
Schmidt et al., have described that adjuvant radio and chemotherapy have resulted in survival rates of more than 3 years in a patient of SCC of stomach. [4]
In one case reported by Yildirim et al., complete remission was achieved with a combination of cisplatin and 5-fluorouracil, in spite of presence of extensive disease. [6]
Though our patient was advised further adjuvant chemotherapy, she refused the same and was subsequently lost to follow-up.
This adds to the existing literature regarding SCC of stomach.
| Acknowledgement | | |
We thank Department of Radiology and senior laboratory technicians Mrs. Ushanandini and Mr. Ramana for their help.
| References | | |
| 1. | Takita J, Kato H, Miyazaki T, Nakajima M, Fukai Y, Masuda N, et al. Primary squamous cell carcinoma of the stomach: A case report with immunohistochemical and molecular biologic studies. Hepatogastroenterology 2005;52:969-74.  |
| 2. | Callacondo D, Ganoza-Salas A, Anicama-Lima W, Quispe-Mauricio A, Longacre TA. Primary squamous cell carcinoma of the stomach with paraneoplastic leukocytosis: A case report and review of literature. Hum Pathol 2009;40:1494-8. |
| 3. | Amuluru K, Gupta H. Primary squamous cell carcinoma of the stomach: A case report. J Gastrointest Cancer 2010;41:24-6. |
| 4. | Schmidt C, Schmid A, Lüttges JE, Kremer B, Henne-Bruns D. Primary squamous cell carcinoma of the stomach. Report of a case and review of literature. Hepatogastroenterology 2001;48:1033-6. |
| 5. | Muto M, Hasebe T, Muro K, Boku N, Ohtsu A, Fujii T, et al. Primary squamous cell carcinoma of the stomach: A case report with a review of Japanese and Western literature. Hepatogastroenterology 1999;46:3015-8. |
| 6. | Yildirim Y, Akcali Z, Bilezikci B, Ozyilkan O. Primary squamous cell carcinoma of the stomach: A case report. Tumori 2005;91:440-2. |
| 7. | Parks RE. Squamous neoplasms of the stomach. Am J Roentgenol Radium Ther Nucl Med 1967;101:447-9. |
| 8. | Boswell JT, Helwig EB. Squamous cell carcinoma and adenoacanthoma of the stomach. A clinicopathologic study. Cancer 1965;18:181-92. |
| 9. | Mori M, Iwashita A, Enjoji M. Squamous cell carcinoma of the stomach: Report of three cases. Am J Gastroenterol 1986;81:339-42. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
[Table 1]
|