|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2013 | Volume
: 15
| Issue : 1 | Page : 17-21 |
|
Causes of visual impairment and blindness in Kaduna State Special Education School
ER Abah1, KK Oladigbolu1, AO Ahmed2
1 Department of Ophthalmology, Ahmadu Bello University Teaching Hospital, Shika-Zaria, Nigeria
2 Department of Otorhinolaringology, Aminu Kano Teaching Hospital, Kano, Nigeria
| Date of Web Publication | 22-Sep-2014 |
Correspondence Address:
E R Abah
Consultant/Senior Lecturer Department of Ophthalmology, Ahmadu Bello University Teaching Hospital, Shika-Zaria
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/1595-1103.141387

Aims and Objectives: To identify the causes of visual impairment and blindness in students of Kaduna State Special Education School (KASSES) and make recommendations for the planning of eye care, including prevention and management of the avoidable causes of childhood blindness in our environment.
Background: Childhood blindness is one of the priorities of vision 2020: The Right to sight. The "blind years" attributable to childhood is comparable to that of age related cataract (the commonest cause of blindness worldwide). Significant proportions of the causes of childhood blindness are avoidable and can be identified after a screening exercise and treated. Periodic screening will also provide current data for planning and implementation of childhood blindness prevention programmes.
Materials and Methods: All the students of the blind section of KASSES who were present during the study were examined and the Georgia Project's screening protocol for visual impairment in children was completed for each of them. The data was analyzed using Analyze-it V2.22 (2010) statistical software.
Results: A total of 71 students were examined. M:F ratio was 1.7:1. The age range was between 6-29 years but 76% were within the bracket of 10-19 years. Seventy percent were blind, 21% had severe visual impairment, and 9% had moderate visual impairment. Cataract was the commonest cause of blindness (25.3%), followed by trauma (16.9%), optic atrophy, buphthalmos, and retinitis pigmentosa (12.7% each). Others were corneal scarring/staphyloma (9.9%), Rubella (7.0%), and a case each of bilateral ankyloblepharon and uveitis (1.4%).
Conclusion: The causes of visual impairment in KASSES are largely avoidable. Incorporation of Primary Eye Care (PEC) into Primary Health Care (PHC) will drastically reduce needless blindness, especially in childhood and the morbidity and mortality associated with the blind years. Early identification of students with treatable causes such as cataract should also be encouraged through regular school screening and health education. Keywords: Childhood blindness, causes, prevention
How to cite this article:
Abah E R, Oladigbolu K K, Ahmed A O. Causes of visual impairment and blindness in Kaduna State Special Education School. Niger J Surg Res 2013;15:17-21 |
How to cite this URL:
Abah E R, Oladigbolu K K, Ahmed A O. Causes of visual impairment and blindness in Kaduna State Special Education School. Niger J Surg Res [serial online] 2013 [cited 2017 Feb 20];15:17-21. Available from: http://www.njsrjournal.org/text.asp?2013/15/1/17/141387 |
| Introduction | |  |
The childhood period (1-15 years) remains the most critical period for the onset of blindness and a significant proportion are due to avoidable causes. [1] There are estimated 1.4 million blind children worldwide out of which about 320,000 live in Sub-Saharan Africa. [2] Childhood blindness is responsible for a high number of "blind years" such that even though the actual number of blind children is much smaller than the number of blind adults, the total "blind years" lived are comparable to those due to age related cataract. Furthermore, blindness in children is related to child mortality. For these reasons, the control of blindness in children is considered a high priority within the World Health Organisation's (WHO) Vision 2020 initiative: The Right to Sight. [3]
There is a wide regional variation in the causes of blindness and in the cause specific prevalence of childhood blindness. Corneal scarring is the most important cause of blindness in children in the low income countries of the world. In high income countries, lesions of the central nervous system (CNS) predominate. In middle income countries the picture is mixed, with retinopathy of prematurity emerging as an important avoidable cause of childhood blindness. In all regions of the world, cataract, retinal diseases, and congenital abnormalities affecting the whole globe are important causes of blindness. [4] Blind school studies [5],[6],[7],[8] indicate that 14-42% of children are blind from entirely preventable causes in Africa, Asia, and Latin America with conditions that can be treated to prevent blindness or restore vision are responsible for further 16-33%. [9]
In developing countries like Nigeria, inadequate medical manpower, a largely rural population, and lack of necessary facilities can result in children becoming blind (or remaining blind) from avoidable causes. [7]
The introduction of Special Education in Nigeria has, to some extent, improved the outlook for some children with severe visual impairment or blindness. However, to the knowledge of the authors, there is no known community based program in Nigeria that screens newborn babies, or screens older children before they are admitted into the blind school. [7] Vision screening before admission into blind school will create more space for children who are incurable by isolating those with curable blindness for treatment. Although some parents/guardians want their children to remain in the blind school because it is a free facility. However, the current practice is inclusive education where blind and sighted children are trained in the same school. Periodic school screenings provide current data for planning and implementation of childhood blindness prevention programs.
| Materials and Methods | | |
KASSES is a state government sponsored mixed special education school located within Kaduna metropolis. It provides special boarding nursery, primary, and junior secondary education for the deaf and primary education for the blind within Kaduna and adjoining states such as Plateau, Nassarrawa, Katsina, Kano, and other parts of the country.
The blind section is a Primary school made up of classes 1-6. A cross sectional study of 91 students in this section was conducted.
All the students who were present in the blind section of the school were evaluated and those who were absent within the period of the study were excluded.
Permission and ethical clearance to conduct the study were obtained from Kaduna State Ministry of Education and Health Research Ethics Committee of Ahmadu Bello University Teaching Hospital, Shika respectively. Written informed consent was obtained from the students.
Two teachers were trained to conduct visual acuity and also to explain and help to complete the questionnaire section of the protocol for the students. Georgian protocol for assessment of visual impairment in children was used to extract information on personal data, medical and surgical history, past ocular history, and family history. Blindness was defined as visual acuity of ≤3/60 in the better eye after refraction and best correction. Severe and moderate visual impairment were defined as corrected visual acuity of <6/60-3/60and < 6/18-6/60, respectively. The visual acuity for distance (6 m) and near (33 cm) was assessed using Snellen's "E" chart and reduced illiterate Snellen's near chart respectively. Anterior segment examination was conducted with pen torch and loupe while the posterior segment examination was done with a direct ophthalmoscope. Dilated fundoscopy with 1% cyclopentolate and 10% phenylepherine was done for those whose fundus could not be readily examined. Ishihara chart was used to assess color vision and all the findings were entered into the protocol. The few whose visual acuity improved slightly with the use of pinhole were refracted. However, there was no remarkable benefit from conventional optical correction so; low vision assessment was conducted by a trained optometrist. Other examinations mentioned were carried out by one of the two Ophthalmologists who conducted the study. These included intraocular pressure check using hand-held Perkins applanation tonometer for those who had suspicious optic discs or obvious optic disc cupping.
The study was conducted within a period of 3 weeks (16 th January-6 th February, 2013 and the data collected was analyzed using Analyze-it V2.22 (2010) statistical software.
| Results | | |
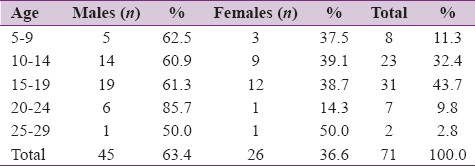
Out of 91 students enrolled into this school, a total of 71 students were examined giving a participation rate of 78.0%. The age range was 6-29 years with mean age of 15 years +/- Standard Deviation (SD) 3.9. There were 45 males and 26 females with M:F ratio of 1.7:1 [Table 1].
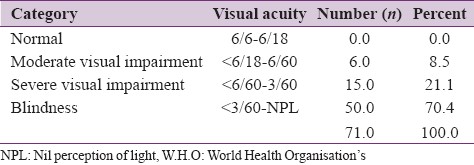
None of the students had normal vision. Those with moderate visual impairment and severe visual impairment constituted 8.5%, n = 6 and 21.5%, n = 15 respectively. Majority of the students were blind, 70.4%, n = 50 [Table 2].
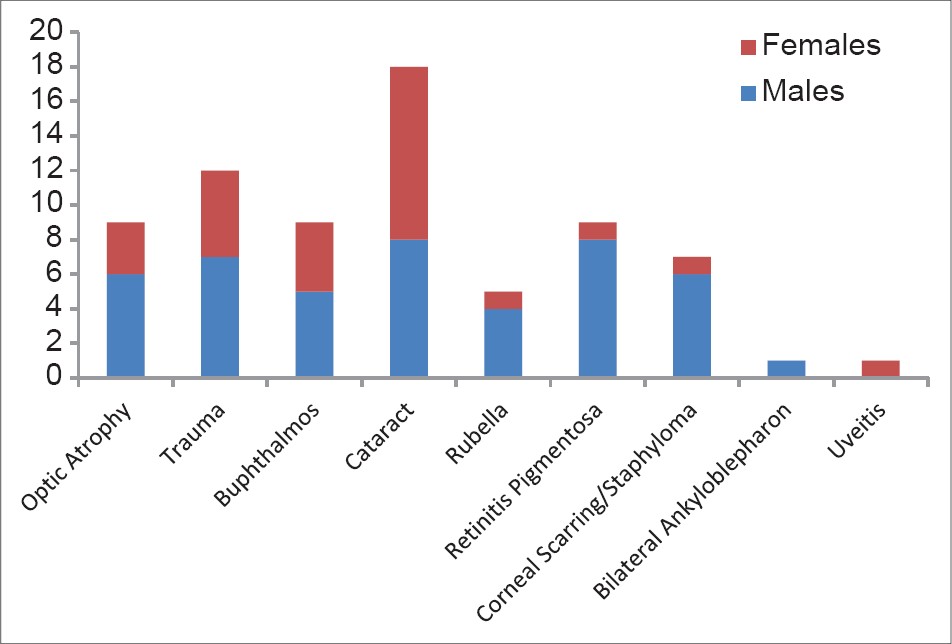
Cataract was responsible for visual loss in most of the students, 25.3% ( n = 18). Trauma was responsible for 16.9% while optic atrophy, retinitis pigmentosa, and buphthalmos accounted for 12.7% each ( n = 9 each). Corneal scarring and rubella were fairly common, 9.9% and 7.0% respectively. Others were a case each of uveitis and bilateral ankyloblepharon [Figure 1].
Cataract which is treatable and corneal scarring (predominantly due to Vitamin A deficiency/measles based on information extracted from the protocol and the scar location) and trauma which are largely preventable make up avoidable blindness [52.1%].
Genetic causes such as Buphthalmos, Optic Atrophy, and Retinitis pigmentosa accounted for 38.1%.
The main anatomical sites affected by the blinding diseases in this study are the lens and the cornea.
Eight pupils had some visual improvement with low vision devices. One, with Χ4 telescope and another seven with Χ6 telescope. The pupil who needed Χ4 telescope had a pre-assessment Visual Acuity (VA) of 6/36-1 in both eyes (BE) which improved to 6/9. She could read N 8 at 10 cm. The other seven had visual improvement from less than a metre in BE to 6/24 with Χ6 telescope except one who improved to 6/18. They could read N14 at 10 cm with 14 dioptre lenses.
| Discussion | | |
Males were almost twice as much as females. This is similar to the results of previous blind school studies in Nigeria, other parts of Africa, Asia, and America. [1],[5],[6],[7],[10],[11],[12],[13],[14],[15] This is probably due to the greater value accorded to the education of male children in this part of the country. While in most western countries including America, hereditary diseases are a significant cause of childhood blindness and are more common in males.
The age range of 6-29 years with a mean of 15 years is suggestive of delayed school entry age either because of the visual handicap, lack of awareness of the availability of special education facility, accessibility or affordability.
Expectedly, most of the students in this school were found to be blind and severely visually impaired (92%). This is similar to the findings in other blind school studies in Nigeria [1] and Indonesia. [11]
No child had normal vision as compared to a previous study in Northern Nigeria that recorded normal vision in 4% of the students studied. [1] The presence of students with normal vision in blind schools is because guardians or parents want their children to benefit from the free education, accommodation, and feeding provided by these schools even though their children are not blind.
Cataract was responsible for visual loss in most of the students (25.3%). This is very close to the finding of previous researchers in Northern Nigeria (29.0%) [1] but higher than that of Western Nigeria (14.3%) [10] where corneal blindness predominated. In Pakistan, retinal diseases were found to be more common (41%) [12] while in Indonesia, corneal diseases were predominant (29.7%). [11] In Ethiopia, cataract was responsible for only 9.2% while corneal scarring made up 62.4%. [13] Corneal scarring was responsible for about 10% of blindness in our study. This may be due to the increased effort of Vitamin A distribution, Expanded Program on Immunization (EPI) against Measles and other diseases and health education against the use of harmful eye preparations or practices. Trauma, optic atrophy, buphthalmos, retinitis pigmentosa, and rubella were fairly common. One student each had chronic anterior uveitis (etiology unknown) and bilateral ankyloblepharon which continues to recur after surgery (was operated twice by another team of doctors).
In studies conducted in Asia, genetic diseases were responsible for 42% of blindness and severe visual impairment in Indonesia, [11] 35.0% in Sri Lanka, [16] 16.8% in Thailand and Philippines, [17] 23.0% in India, [18] 30.7% in China, [19] and in Malaysia it was 29.5%. [20] In our study, it was responsible for 38.1%, which is similar to the findings of the above studies. In high-income countries such as United Kingdom [21] and United States [17] , blindness related to perinatal diseases such as Retinopathy of Prematurity (ROP), were the predominant cause of blindness and severe visual impairment. In addition to ROP, the leading cause of paediatric blindness in the United States is cortical visual impairment [15] and optic nerve disorders. [15],[17] In our study, perinatally related diseases, such as ROP, were not identified in any patient. The absence of ROP in our study is probably as a result of the much higher mortality of premature children in Nigeria because of limited facilities for neonatal care, particularly in rural areas, compared to developed countries. Most students in the blind school were born and spent their childhood in rural areas. In the future, ROP is likely to become a much bigger problem in Nigeria, as neonatal care services are expected to improve, particularly in urban areas.
In general, optic nerve and visual pathway lesions predominate as cause of blindness in high-income countries, [15],[16],[17] while corneal scarring (due to Measles and Vitamin A deficiency, harmful eye remedies, and Ophthalmia neonatorum) is a major cause in low income countries. [16],[18] In all countries, cataract and hereditary retinal dystrophies are fairly common. [22],[23],[24],[25],[26]
The main anatomical sites of abnormality leading to severe visual impairment or blindness among the students were the lens and cornea. This was reported in similar studies in the past within the country. [1],[7],[8]
The preventable (corneal scarring from Vitamin A deficiency and measles, harmful eye medications and trauma) and the treatable (cataract) childhood eye diseases which comprises of avoidable blindness, contributed about 50% of the cases unlike the 70% reported in other local studies. [1],[7],[8] Probably because of interventions at primary health care level (vaccination against measles, mass chemotherapy with vitamin A, and health education); secondary and tertiary health care levels (improved cataract surgical rate).
Optical or low vision assessment is rewarding. One of the pupil's visual acuity improved from 6/36-1 to 6/9 in both eyes. This pupil could be integrated into a conventional school with a Χ4 telescope. Seven others also had remarkable visual improvement with low vision devices and this could improve their quality of life and learning ability.
| Limitations | | |
Although blind school studies provide access to large number of blind students at a time, the extrapolation of the conclusion drawn from their study is limited by its school setting, small sample size, inherent unreliability of student-reported data and lack of modern diagnostic facilities available to the researcher. A larger sample size, multicentre design preferably cross- sectional is suggested.
| Conclusion/Recommendation | | |
The major causes of blindness among the students were cataract, trauma, genetic diseases such as retinitis pigmentosa, and corneal scarring (from vitamin A deficiency/measles and harmful traditional eye preparations/practices). Some of these are either preventable (corneal scarring) or treatable (cataract), both constitute avoidable blindness.
A good number of those with cataract may benefit from cataract surgery. The services of Paediatric Ophthalmologists in accessible, affordable, well equipped specialist centres will be required to achieve this. So, there is need for subspecialty training in this area, more so that childhood blindness is a priority in World Health Organization's Global Initiative for the elimination of avoidable blindness by 2020. [16],[27],[28]
Blindness from corneal scarring appears to have dropped because of interventions (vitamin A distribution, EPI, health education/nutrition, and breast feeding practices etc.) but there is need to extend these to the remote areas. Incorporation of PEC into the existing PHC structure will facilitate the control of these blinding diseases. Regular school eye screening will ensure early identification and treatment of childhood blinding diseases.
Genetic counselling to discourage consanguineous marriage and educate individuals about hereditary diseases and their mode of transmission should be intensified. Centres should be available for detailed genetic studies to aid more precise diagnosis of these inherited disorders.
Optical or low vision services should also be available to maximise rehabilitation of the students so that they can live independently and interact freely with their sighted peers.
| Acknowledgement | | |
We wish to thank Dr Bagaiya T for taking his time to perform low vision assessment for the pupils. In the same vain we would like to thank the school authority and the teachers, especially Abubakar TH who helped in the interpretation of the protocol, visual acuity assessment and other logistics.
| References | | |
| 1. | Odugbo OP. Blind school survey in Plateau, Bauchi and Kaduna states. J Comm Eye Health 2005;18:130-134. 
|
| 2. | World Health Organization. Preventing blindness in children. A report of WHO/IAPB scientific meeting. WHO/PBL/00.77. Vol. 1. Geneva: WHO; 2000. p. 33.
|
| 3. | World Health Organization. Global initiative for the elimination of avoidable blindness. WHO/PBL/97.61. Vol. 2. Geneva: WHO; 1997. p. 17-19.
|
| 4. | Gilbert C. New issues in childhood blindness. J Comm Eye Health 2001;14:53-6.
|
| 5. | Wolde-Gabriel Z, Gerbu H, West CE. Causes of blindness in children in blind schools in Ethiopia. Trop Geogr Med 1992;44:135-41.
|
| 6. | Chirambo MC, Benexra D. Causes of blindness among students in blind school institution in developing country. Br J Ophthalmol 1976;60:665-8.
|
| 7. | Umeh RE, Chukwu A, Okoye O, Cookey-Gam DC, Onwasigwe EN. Treatable causes of blindness in a school for the blind in Nigeria. J Comm Eye Health 1997;10:14-5.
|
| 8. | Akinsola FB, Ajaiyeoba AI. Causes of low vision and blindness in children in a blind school in Lagos, Nigeria. West Afr J Med 2002;21:63-5.
|
| 9. | Wormald R. Screening in ophthalmology. In: Johnson GJ, Minssian DC, Weale R, (eds.) The Epidemiology of Eye Diseases. London: Chapman and Hall Medical; 1998. p. 83-100.
|
| 10. | Ajibode HA, Onabolu OO, Oluyadi FO. Causes of blindness among blind students in Ogun state, Nigeria. Nig J Clin Pract 2003;6:17-9.
|
| 11. | Sitorus R, Presing M, Lorenz B. Causes of blindness at "Wiyata Guna" School for the blind, Indonesia. Br J Ophthalmol 2003;87:1065-8.
|
| 12. | Khan SJ, Hassan A, Khalid L, Karim U, Hashmi E, Gul F, et al. Blindness in children at the Ida Rieu School for the blind and deaf. J Pak Med Assoc 2007;57:334-7.
|
| 13. | Kello AB, Gilbert C. Causes of severe visual impairment and blindness in children in schools for the blind in Ethiopia. Br J Ophthalmol 2003;87:526-30.
|
| 14. | Merin S, Lapithis AG, Horovitz D, Michaelson IC. Childhood blindness in Cyprus. Am J Ophthamol 1972;74:538-42.
|
| 15. | DeCarlo DK, Nowakowski R. Causes of visual impairment among students at Alabama school for the blind. J Am Optom Assoc 1999;70:647-52.
|
| 16. | Gilbert C, Foster A. Childhood blindness in the context of vision 2020--the right to sight. Bull World Health Organ 2001;79:227-32.
|
| 17. | Steinkuller PG. Du L, Gilbert C, Foster A, Collins ML, Coats DK. Childhood blindness. J AAPOS 1999;3:26-32.
|
| 18. | Rahi JS, Sripathi S, Gilbert CE, Foster A. Childhood blindness in India: Causes in 1318 blind school students in nine states. Eye (Lond) 1995;9:545-50.
|
| 19. | Hornby SJ, Xiao Y, Gilbert CE, Foster A, Wang X, Liang X, et al. Causes of childhood blindness in the people's republic of China. Results from 1131 blind school students in 18 provinces. Br J Ophthalmol 1999;83:929-32.
|
| 20. | Reddy SC, Tan BC. Causes of childhood blindness in Malaysia: Results from a national study of blind school students. Int Ophthalmol 2002;24:53-9.
|
| 21. | Alagaratnam J, Sharma TK, Lim CS, Fleck BW. A survey of visual impairment in children attending the Royal Blind School, Edinburg using the WHO childhood visual impairment data base. Eye (Lond) 2002;16:557-61.
|
| 22. | Lewallen S, Courtright P. Blindness in Africa: Present situation and future needs. Br J Ophthalmol 2001;85:897-903.
|
| 23. | Eckstein MB, Foster A, Gilbert CE. Causes of childhood blindness in Sri Lanka. Results from children attending six schools for the blind. Br J Ophthamol 1995;79:633-6.
|
| 24. | Baghdassarian SA, Tabbara KT. Childhood blindness in Lebanon. Am J Ophthalmol 1975;79:827-30.
|
| 25. | Tabbara KF, Badr IA. Changing pattern of childhood blindness in Saudi Arabia. Br J Ophthalmol 1985;69:312-5.
[PUBMED] |
| 26. | Hamamy H, Alwan A. Hereditary disorders in the Eastern Mediterranean region. Bull World Organ 1994;72:145-54.
|
| 27. | Gibert C, Foster A, Negrel AD, Thylefors B. Childhood blindness: A new form for recording causes of visual loss in children. Bull World Health Organ 1993;71:485-9.
|
| 28. | Thylefors B. A global initiative for the elimination of avoidable blindness. Am J Ophthalmol 1998;125:90-3.
[PUBMED] |
[Figure 1]
[Table 1], [Table 2]
|









 Search Pubmed for
Search Pubmed for