|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2013 | Volume
: 15
| Issue : 1 | Page : 13-16 |
|
Ultrasound-guided percutaneous drainage of liver abscess: 6 years experience in Lagos State university teaching hospital, Lagos
BO Balogun1, OO Olofinlade1, R Igetei2, CA Onyekwere2
1 Department of Radiology, Lagos State University Teaching Hospital, Lagos, Nigeria
2 Department of Medicine, Lagos State University Teaching Hospital, Lagos, Nigeria
| Date of Web Publication | 22-Sep-2014 |
Correspondence Address:
B O Balogun
Department of Radiology, Lagos State University, College of Medicine, Ikeja, Lagos
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/1595-1103.141386

Introduction: Liver abscesses, both amoebic and pyogenic, continue to be an important cause of morbidity and mortality in tropical countries. The management has improved significantly over the years with the advent of potent antimicrobial agents and advances in diagnostic imaging.
Materials and Methods: From August 2007 to May 2013, 32 patients with liver abscess were referred to the Department of Radiology, Lagos University Teaching Hospital, Lagos, Nigeria for ultrasound-guided percutaneous aspiration or drainage. All patients had been treated with antibiotics or antimicrobials for at least 2 weeks before referral and were still being continued for another 6 weeks.
Results: A total of 32 patients with liver abscess were successfully treated, consisting 31 males and 1 female. The age ranged from 2 to 72 years with a mean of 43.6 years. A total of -22 (68.75%) patients had percutaneous catheter drainage, while 12 (31.25%) had percutaneous needle aspiration. A total of 15 (46.87%) patients had single abscess, while 5 (15.63%) had two and 12 (37.50%) had more than 2. Most of the abscesses are located on the right in 25 (78.12%). One needle insertion was used per patient. The amount of aspirated pus ranged from 100 to 3000 mL with a mean of 850 mL. Only 10 (31.25%) patients were on admission at the time of drainage, while the others 22 (68.75%) were day cases.
Conclusion: We found that needle aspiration and catheter drainage when combined with chemotherapy represents a successful therapeutic approach in the treatment of liver abscess whether pyogenic or amoebic. Keywords: Antibiotics, catheter drainage, interventional radiology, liver abscess, needle aspiration, sonography
How to cite this article:
Balogun B O, Olofinlade O O, Igetei R, Onyekwere C A. Ultrasound-guided percutaneous drainage of liver abscess: 6 years experience in Lagos State university teaching hospital, Lagos. Niger J Surg Res 2013;15:13-6 |
How to cite this URL:
Balogun B O, Olofinlade O O, Igetei R, Onyekwere C A. Ultrasound-guided percutaneous drainage of liver abscess: 6 years experience in Lagos State university teaching hospital, Lagos. Niger J Surg Res [serial online] 2013 [cited 2017 Feb 5];15:13-6. Available from: http://www.njsrjournal.org/text.asp?2013/15/1/13/141386 |
| Introduction | |  |
Liver abscesses, both amoebic and pyogenic, continue to be an important cause of morbidity and mortality in tropical countries. [1] The management has improved significantly over the years with the advent of potent antimicrobial agents and advances in diagnostic imaging. In the past 3 decades, image-guided percutaneous needle aspiration (PNA) or catheter drainage (PCD) has become the therapy of choice for liver abscess. [2],[3]
This minimally invasive approach has high clinical success rate, low complication rate, and avoids general anaesthesia and its attendant risk. [4],[5]
The advantage of sonographic over computed tomography (CT) guidance is that sonography is real-time imaging technique that allows monitoring of the course of the needles and catheter as they traverse tissues. [6]
To our knowledge, in our environment, not much data are available on large series of patient with liver abscess managed sorely with PNA or PCD under ultrasound guidance in combination with long-term antibiotic treatment. We, therefore, report our experience in the management of liver abscess using both methods in Lagos State University Teaching Hospital Lagos, Nigeria.
| Materials and Methods | | |
From August 2007 to May 2013, 32 patients with liver abscess were referred to the Department of Radiology, Lagos State University Teaching Hospital, Lagos, Nigeria for ultrasound-guided percutaneous aspiration or drainage (31 males and 1 female). All patients had been treated with antibiotics or antimicrobials for at least 2 weeks before referral and were still being continued during and after drainage for another 6 weeks by the referring physician. The patients had been diagnosed for liver abscess previously using either ultrasound scan or CT scan. Informed consent was obtained from the patients.
This retrospective study was approved by the institution ethics committee.
All the aspiration procedures were performed under sonographic guidance using a free hand technique. The machine used is GE LOGIQ 5 Expert or Mindray (model DP-6600) ultrasound machines with dual probes (3.5 and 7.5 MHz).
Local anesthesia was induced with 10 mL of lidocaine hydrochloride 2%. In young children the so called conscious sedation was used with intravenous injection of pentazocine and diazepam. Then continuous real-time sonographic imaging was used to localize the abscess and to guide insertion of the needle.
18 - 20G, 20 cm Chiba needle was used for needle aspiration in small abscesses (<500 mL). In some with multiple abscesses, the same needle was reinserted into several surrounding loculi to aspirate pus. After successful puncture, a sample of fluid was sent for bacterial culture and sensitivity. The decision to place a drain was made depending on the size of collection. Catheter drainage was used for large abscesses greater than 500 mL (> 8cm in diameter) and in most of the children.
Catheter insertion into the abscess cavity was done using Seldinger's technique. (A percutaneous nephrostomy puncture set by Urotech, Germany was used) [Figure 1]. Most of the pus was usually drained off actively on the same day, while the catheter is left in situ for any remnant to drain into the attached bag.
In more viscous pus, the cavity was washed with about 20-50 mL of sterile hypertonic solution injected slowly into the abscess and left in place for 1-2 h before reaspiration is done.
The PNA or PCD was considered successful when the cavity collapses or was reduced to below 20 mL with no relapse of abscess [Figure 2]. | Figure 2: Sonogram of the liver with a drainage catheter, in a collapsed abscess cavity
Click here to view |
Follow-up of patients on catheter was done daily until catheter was removed. Thereafter, all patients were seen 1 week after aspiration for follow-up sonography. The patients were then being managed by their respective doctors until stability of all the clinical indices before been discharged.
| Results | | |
A total of 32 patients with liver abscess were successfully treated, consisting 31 males and one female.
The age ranged from 2 to 72 years with a mean of 43.6 years. A total of 22 (68.75%) patients had PCD, while 10 (31.25%) had PNA. A total of 15 (46.87%) patients had single abscess [Figure 3], while 5 (15.63%) had two and 12 (37.50%) had more than 2. Most of the abscesses are located on the right in 25 (78.1%). One needle insertion was used per patient. The amount of aspirated pus ranged from 100 to 3000 mL with a mean of 850 mL. A total of 14 (43.75%) patients have aspirated fluid less than 500 mL (small abscesses), while 18 (56.25%) have more than 500 mL (large abscesses). The average duration of aspiration of fluid range from 1 to 8 h with a mean of 2 h. The patient with 3000 mL of pus was done over a period of 4 days with a total aspiration time of 8 h. Only 10 (31.25%) patients were on admission during the time of drainage, while the others 22 (68.75%) were day cases. | Figure 3: Sonogram of the liver showing a single abscess cavity in the right lobe
Click here to view |
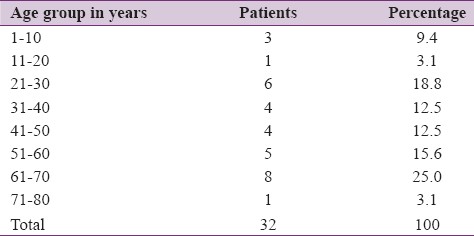
The age group with the highest incidence of abscess was in the (61 - 70) group with 25.0% [Table 1] closely followed by the (21 - 30) group with 18.75%.
Of the 32 patients treated, 6 (18.7%) had amoebic abscess with typical anchovy sauce fluid drained from them, while 26 (81.3%) had pyogenic liver abscess with whitish to yellowish fluid.
On the basis of sensitivity and culture, most of the pus from pyogenic abscess did not yield any organism. In 6 (18.7%) samples, Escherichia coli was cultured, while 2 (6.3%) had Klebsiella species.
PNA and PCD were successful in all the patients. No major complications were seen. Minor complications include mild pain at the hypochondrium and mild bleeding during needle insertion. One (3.12%) patient with pyogenic abscess had a repeated aspiration because he was not complying with drugs prescribed by the referring physician.
However, two patients died in the immediate postaspiration days. One was a 4 years old, male, acute leukaemia patient with pyogenic abscess who died 3 days after aspiration. The cause of death was not established. The other was a 72-year-old, male patient, who had thick pus and cultured E. coli but died of thromboembolism a week later.
The only female patient belonged to the pyogenic group but was found to also have an ovarian cyst.
| Discussion | | |
Controversies still exist in the management of liver abscess. [7] Percutaneous drainage (either needle aspiration or catheter drainage) coupled with systemic antibiotics has become the preferred treatment for the management of pyogenic abscess. [3],[4],[8] In contrast, for amoebic abscesses, the primary mode of treatment is medical; however, as many as 15% may be refractory to medical therapy. Also secondary bacterial nfection may complicate 20% of amoebic liver abscess. [3]
We found percutaneous drainage of liver abscess an easy and effective method of treatment. It was effective in evacuating the abscess in all the patients studied. Our method involved active drainage of most abscess cavities even with catheter drainage until the cavity collapses. The residual is then left to drain into the attached bag for the next 2 days before removal.
Our study records high cases of pyogenic (81.3%) over amoebic abscesses with (18.7%) notwithstanding a high prevalence of amoebiasis in tropical Africa. This is in contrast with similar work done by Singh et al0.,[9] in the tropics with 67% amoebic and 37% pyogenic.
Age group (61 - 70) has the highest incidence in our study consisting of 25.0%. This is in contrast with similar works done by Mgbor et al.,[10] and Mukhopadhyay et al.,[11] where the highest incidence was in the age group (31×40). However, Baig et al.,[12] noted a change in pattern to the 5 th decade probably due to changing etiology from suppurative appendicitis to hepatobiliary causes. However, we did not see any associated hepatobiliary disease in our study.
Male predominance may be attributed to the lifestyle of man and women of this country with men folk going out to work and consuming contaminated water and unhygienic food from street vendors and road side eateries, while the women are largely confined to their homes
In the last decade, diagnostic imaging has played a major role in early diagnosis of liver abscess and due to advances in the field of ultrasonography it has become a standard practice for detection of liver abscess. Nevertheless, not many centers are involved in the percutaneous drainage of liver abscess possibly due to nonavailability of suitable percutaneous drainage sets. Previous studies have seen the use of Foley's catheter as drainage tubes. [13] Some researchers have constructed the ''UNICAL DRAIN'' a closed drainage system. [14] In our study, we adapted a percutaneous nephrostomy set which is readily available.
Complications have been reported with both catheter drainage [4] and needle aspiration. [15] Our study and some recent reports suggest that both procedures if properly performed are essentially safe procedures with minimal complications.
The main limitation of our study is the inability to determine causative organism in most of the pyogenic abscesses. A major drawback is our inability to carry out serology investigations on the patients, resulting in patients with amoebic abscess and possibly secondary pyogenic infection been missed. Our institution is a referral centre and many of these patients had been partially treated with both antibiotics and antimicrobial drugs. This probably accounts for the high percentage of abscesses with negative findings on pus cultures in our study. Some previous researchers have also had this experience. [2],[3]
Relatively large abscess cavities were seen in this study with mean pus volume of 850 mL, but with early diagnosis and prompt treatment coupled with chemotherapy and percutaneous drainage, low morbidity and mortality will likely result.
| Conclusion | | |
This study represents our preliminary work on liver abscess drainage. We found that needle aspiration and catheter drainage when combined with chemotherapy represents a successful therapeutic approach in the treatment of liver abscess whether it is pyogenic or amoebic.
| References | | |
| 1. | Sharma N, Sharma A, Varma S, Lal A, Singh V. Amoebic liver abscess in the medical emergency of a North Indian hospital. BMC Res Notes 2010;3:21. 
|
| 2. | vanSonnenberg E, Mueller PR, Schiffman HR, Ferrucci JT Jr, Casola G, Simeone JF, et al. Intrahepatic amebic abscesses: Indications for and results of percutaneous catheter drainage. Radiology 1985;156:631-5.
[PUBMED] |
| 3. | Rajak CL, Gupta S, Jain S, Chawla Y, Gulati M, Suri S. Percutaneous treatment of liver abscesses: Needle aspiration versus catheter drainage. AJR Am J Roentgenol 1998;170:1035-9.
|
| 4. | Lambiase RE, Deyoe L, Cronan JJ, Dorfman GS. Percutaneous drainage of 335 consecutive abscesses: Results of primary drainage with 1-year follow-up. Radiology 1992;184:167-79.
|
| 5. | Giorgio A, Tarantino L, Mariniello N, Francica G, Scala E, Amoroso P, et al. Pyogenic liver abscesses: 13 years of experience in percutaneous needle aspiration with US guidance. Radiology 1995;195:122-4.
|
| 6. | Giorgio A, de Stefano G, Di Sarno A, Liorre G, Ferraioli G. Percutaneous needle aspiration of multiple pyogenic abscesses of the liver: 13-year single-center experience. AJR Am J Roentgenol 2006;187:1585-90.
|
| 7. | Arshad Z, Saijad A. Amoebic liver abscess: A comparative study of needle aspiration versus conservative treatment. J Ayub Med Coll Abottabad 2002;14:10-2.
|
| 8. | Yu SC, Ho SS, Lau WY, Yeung DT, Yuen EH, Lee PS, et al. Treatment of pyogenic liver abscess: Prospective randomized comparison of catheter drainage and needle aspiration. Hepatology 2004;39:932-8.
|
| 9. | Singh O, Gupta S, Moses S, Jain DK. Comparative study of catheter drainage and needle aspiration in management of large liver abscesses. Indian J Gastroenterol 2009;28:88-92.
|
| 10. | Mgbor SO, Eke CI, Onuh AC. Amoebic liver abscess: Sonographic patterns and complications in Enugu, Nigeria. West Afr J Radiol 2003;10:8-14.
|
| 11. | Mukhopadhyay M, Saha AK, Sarkar A, Mukherjee S. Amoebic liver abscess: Presentation and complications. Indian J Surg 2010;72:37-41.
|
| 12. | Baig A, Ishaq M, Kumar A, Sheikh M. Pyogenic liver abscess: A five year retrospective study in slums of Karachi. JLUMHS 2012;11:19-23.
|
| 13. | Egba R, Asuquo M, Ugare GU, Udoh I. Closed drainage of liver abscesses: The 'UNICAL' drain as an efficient and cost saving device in a tropical setting. Niger J Clin Pract 2008;11:396-9.
[PUBMED] |
| 14. | Misauno M, Sule A, Ale A, Isichei M. Percutaneous ultrasound guided drainage of abdominal abscesses. Int J Med Imaging 2013;1:23-5.
|
| 15. | Baek S, Lee M, Cho K, Lee SC, Sung KB, Auh YH. Therapeutic percutaneous aspiration of hepatic abscesses: Effectiveness in 25 patients. AJR Am J Roentgenol 1993;160:799-802.
|
[Figure 1], [Figure 2], [Figure 3]
[Table 1]
|










 Search Pubmed for
Search Pubmed for