|
 
 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 16
| Issue : 1 | Page : 23-25 |
|
A huge mesenteric lymphangioma of the jejunal mesentery resulting in failure to thrive
Minakshi Bhosale, Dasmit Singh
Department of Pediatric Surgery, B. J. Government Medical College, Pune, Maharashtra, India
| Date of Web Publication | 8-Oct-2015 |
Correspondence Address:
Minakshi Bhosale
G/101, Sudarshan Apartments, Behind Spencer?fs Daily, Karvenagar, Pune - 411 052, Maharashtra
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/1595-1103.166883

Mesenteric lymphangiomas are rare in occurrence. The dumb-bell shaped ones are even rarer. We report a case of a 7-year-old girl with a huge dumb-bell shaped mesenteric tumor weighing 3 kg, located in the jejunal mesentery and causing failure to thrive. En mass excision of the tumor along with the involved bowel segment was done with a successful outcome. Histopathology diagnosed the tumor to be mesenteric lymphangioma of the jejunal mesentery. At a follow-up of 2 years, the child is symptom-free and has a good catch up growth. Keywords: Child, failure to thrive, jejunum, mesenteric lymphangioma
How to cite this article:
Bhosale M, Singh D. A huge mesenteric lymphangioma of the jejunal mesentery resulting in failure to thrive. Niger J Surg Res 2015;16:23-5 |
| Introduction | |  |
Lymphatic cysts of the mesentery (lymphangiomas) are rare, intra-abdominal masses.[1],[2] Approximately, one-third of the lesions are noted in children.[1] They have a varied presentation, ranging from an asymptomatic mass to acute abdomen.[2] They may present incidentally, insidiously, or as an acute life-threatening emergency. Absence of typical signs and symptoms and characteristic clinical findings makes the diagnosis difficult.
| Case Report | | |
A 7-year-old female child was brought with history of gradually increasing abdominal distension over 2 years. There was no vomiting or constipation. The child was never hospitalized before and no radiological investigations were carried out so far. She was esthetically built and had a weight of 12 kg. The abdomen was massively distended. A vaguely palpable lump was felt on per abdominal examination. It was dull to percussion. Rectal examination was noncontributory. Erect X-ray abdomen showed few gas-filled bowel loops mainly on the left side. Computerized tomography scan of the abdomen was suggestive of a single well-defined nonenhancing lesion with thin walls and internal septations; filling up the entire abdomen and extending onto the pelvic cavity [Figure 1]. It had displaced the bowel loops completely on one side. No other cystic lesions were noted. The kidneys, spleen and ovaries appeared normal. In view of the examination findings and radiologic evaluation, the working diagnosis was that of an omental cyst (lymphangioma).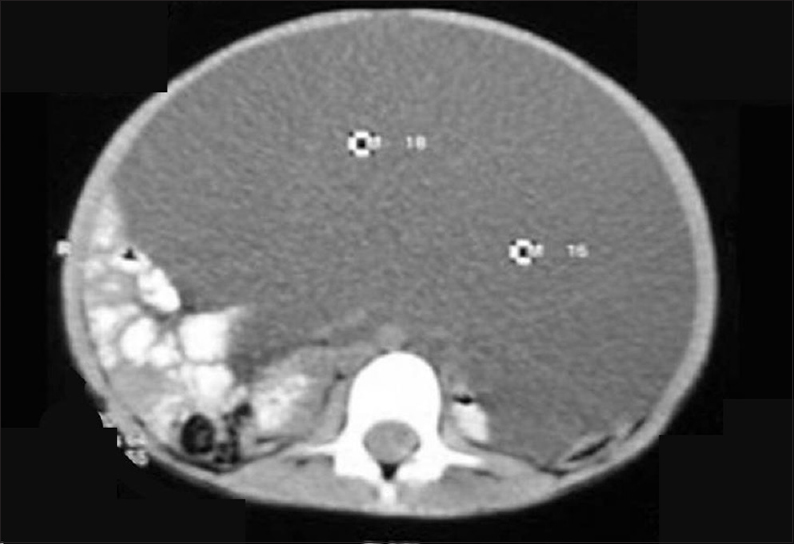 | Figure 1: Computerized tomography scan of the abdomen showing a well-.defined nonenhancing lesion filling up the entire abdomen
Click here to view |
However, on exploration, a 25 cm × 20 cm × 18 cm sized cyst was found within the mesentery of jejunum with completely stretched out overlying bowel segment [Figure 2]. The mass was suggestive of a dumb-bell shaped mesenteric tumor. The surrounding bowel loops were also collapsed because of extrinsic compression.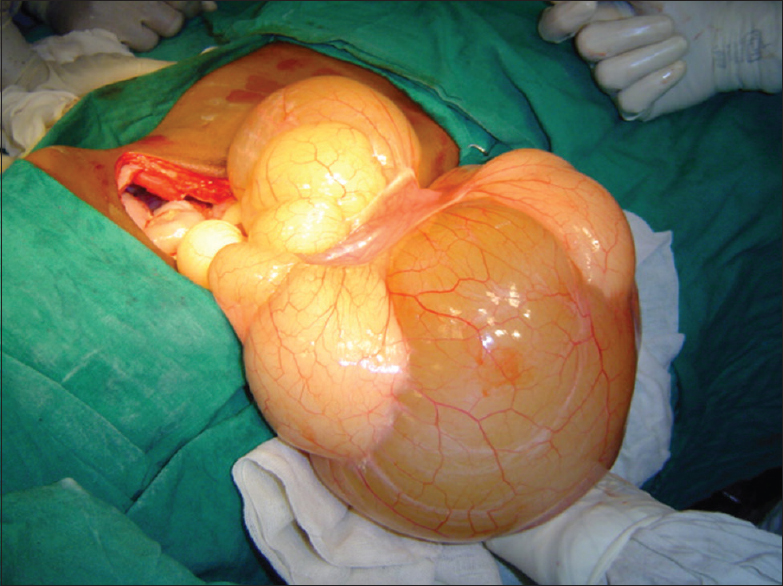 | Figure 2: Large dumb-bell shaped mesenteric tumor with stretched out overlying jejunal segment
Click here to view |
In view of the large size of the tumor, en mass excision of the tumor along with the involved bowel segment was done. Bowel continuity was established by means of interrupted, extramucosal sutures (single layer) using 4-0 polyglactin. The postoperative course was uneventful. Oral feeds were started from postoperative day 6 and were well tolerated. The excised tumor weighed 3 kg. Histopathology showed flattened endothelium without smooth muscle in the cyst wall. Presently, at a follow-up of 2 years, the child is totally asymptomatic and is growing well. She has gained 5 kg weight. The abdomen is scaphoid and there is no radiological evidence of tumor recurrence.
| Discussion | | |
Mesenteric cysts are rare intra-abdominal masses with very sparse literature available in the standard textbooks. Because of their rarity, lack of adequate information, and uniform nomenclature, they have been described differently in various reports presented. Furthermore, there is a lack of a standard classification. In their review article published in the year 2000, de Perrot et al.[3] have put forth a simple and comprehensive classification of intra-abdominal masses based on histopathological features. It categorizes them into the following six groups: Cysts of lymphatic origin (simple lymphatic cyst and lymphangioma), cysts of mesothelial origin (simple mesothelial cyst, benign cystic mesothelioma, and malignant cystic mesothelioma), cysts of enteric origin (enteric cyst and enteric duplication cyst), cysts of urogenital origin, mature cystic teratoma (dermoid cysts), and pseudocysts (infectious and traumatic cysts).[3]
Cysts of lymphatic and mesothelial origin are those most frequently encountered, but both have distinctive clinical features. Lymphangiomas predominate in male children under 5 years of age.[3],[4],[5] Their reported incidence is <1/1,00,000 hospital admissions.[5] They present with chronic abdominal distension or acute intestinal obstruction with or without peritonitis.[4] Lymphatic cysts in the distal small bowel and colonic mesentery contain serous fluid, whereas those located more proximally (proximal small bowel mesentery) are chylous in nature. Although the exact etiology of mesenteric lymphangioma is unknown, their occurrence in neonates and infants supports the theory that they are primary congenital malformations.[5] Stemming from sequestration of the lymphatic tissue, they characteristically infiltrate the surrounding structures by local extension and can produce new lesions by extension or new growth.[6] Radical removal of the tumor with microscopically clear borders is thought to be curative.[7]
In our case, the preoperative diagnosis was that of an omental lymphangioma since the radiological investigations showed a huge cyst in front of the intestines. However, a large dumb-bell shaped mesenteric tumor almost prolapsed out, on opening the abdomen. The overlying portion of the bowel was completely stretched out over the tumor. In view of the gigantic size of the tumor, enucleation was not attempted. Resection of the dumb-bell shaped mass with adherent portion of the intestine was done. The tumor was filled with milk-cream thick chyle [Figure 3], which is the typical presentation of mesenteric lymphangioma. | Figure 3: Excised specimen of the mesenteric tumor (lymphangioma) filled with milk cream thick chyle
Click here to view |
Weeda et al. have reported two cases of mesenteric cystic lymphangiomas in combination with malrotation and intermittent volvulus. Both mesenteric cystic lymphangiomas were located near the duodenojejunal junction.[8] Similarly, in our case, the lymphangioma was located in the proximal jejunal mesentery. However, there was no evidence of malrotation. Contrary to the common occurrence in boys under the age of 5 years, in our case, it presented in a girl child that too at the age of 7 years with failure to thrive.
The report highlights the need for early radiological evaluation of any child presenting with abdominal distension with or without abdominal pain, before catastrophic complications such as volvulus and gangrene of the involved bowel occur. Mesenteric lymphangiomas should be considered as one of the differential diagnoses in children with abdominal pain, particularly after exclusion of more common diagnoses. It attests the age-old assumption that abdomen is still a Pandora's box, in spite of all the modern radiological imaging modalities. The operating surgeon should be aware of all the possible treatment options and should be able to take the right decision on table.
| References | | |
| 1. | Bliss DP Jr, Coffin CM, Bower RJ, Stockmann PT, Ternberg JL. Mesenteric cysts in children. Surgery 1994;115:571-7.  |
| 2. | Prakash A, Agrawal A, Gupta RK, Sanghvi B, Parelkar S. Early management of mesenteric cyst prevents catastrophes: A single centre analysis of 17 cases. Afr J Paediatr Surg 2010;7:140-3. [ PUBMED]  |
| 3. | de Perrot M, Bründler M, Tötsch M, Mentha G, Morel P. Mesenteric cysts. Toward less confusion? Dig Surg 2000;17:323-8. |
| 4. | Steyaert H, Guitard J, Moscovici J, Juricic M, Vaysse P, Juskiewenski S. Abdominal cystic lymphangioma in children: Benign lesions that can have a proliferative course. J Pediatr Surg 1996;31:677-80. |
| 5. | Umap PS. Intra-abdominal cystic lymphangioma. Indian J Cancer 1994;31:111-3. [ PUBMED] |
| 6. | Feins NR. Lymphatic disorders. In: O'Neill JA Jr, Rowe MI, Grosfeld JL, Fonkalsrud EW, Coran AG, editors. Pediatric Surgery. 5 th ed. St. Louis: Mosby; 1998. p. 1973-4. |
| 7. | Losanoff JE, Kjossev KT. Mesenteric cystic lymphangioma: Unusual cause of intra-abdominal catastrophe in an adult. Int J Clin Pract 2005;59:986-7. |
| 8. | Weeda VB, Booij KA, Aronson DC. Mesenteric cystic lymphangioma: A congenital and an acquired anomaly? Two cases and a review of the literature. J Pediatr Surg 2008;43:1206-8. |
[Figure 1], [Figure 2], [Figure 3]
|









 Search Pubmed for
Search Pubmed for