|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 16
| Issue : 1 | Page : 3-10 |
|
Soft tissue sarcoma of the orofacial region: Our experience with 64 cases
Benjamin Fomete1, JO Ogbeifun2
1 Department of Maxillofacial Surgery, Maxillofacial Unit, Ahmadu Bello University Teaching Hospital, Zaria, Kaduna State, Nigeria
2 Department of Dental and Maxillofacial, Federal Medical Centre, Makurdi, Benué State, Nigeria
| Date of Web Publication | 8-Oct-2015 |
Correspondence Address:
Benjamin Fomete
Maxillofacial Unit, Ahmadu Bello University Teaching Hospital, Zaria, Kaduna State
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/1595-1103.166882

Introduction: Soft tissue sarcomas (STSs) are solid malignancies mostly of mesodermal origin whose rarity and variety present formidable challenges in characterization and treatment. According to Pisters and Brennan, STS make up <1% of all oral malignancies. Like other tumors, they can occur at any anatomical site and at any age. The extremities and trunk are favored sites for occurrence and only about 5–10% of STS occur in the head and neck region. STS have varied cell origin, but all STS are considered as a group because of the similarities in their clinical features, natural history, treatment, and disease outcome.
Patients and Methods: Medical records of patients with histopathologically diagnosed malignant oral and maxillofacial tumors between January 2003 and December 2013 were retrospectively reviewed at the Maxillofacial Unit, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria.
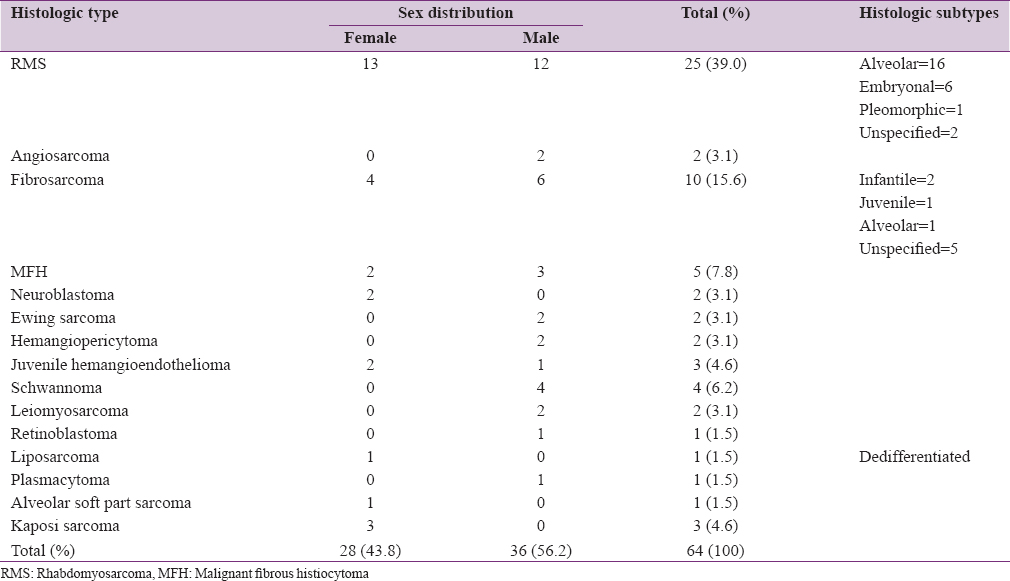
Results: There were more male than female in a ratio of 1.28:1.The age range from 7 months to 70 years with a mean of 29.3 years and 37.8% being <20 and about 62.2% being above 20 years. Rhabdomyosarcoma was the most common lesion (39%) followed by fibrosarcoma (15.6%), malignant fibrous histiocytoma (7.8%). The most common site was the mandible followed by the cheek, palate, and maxilla. Some patients had both mandible and cheek involved while other had both palate and maxilla involved. The most frequent mode of treatment was surgery followed by radio and chemotherapy. A few patients declined therapy.
Conclusion: STS remains a challenge in our center due to late presentation and affordability of treatment by our patients. Another contributing factor is the believe that cancer cannot be treated with orthodox medicine. Keywords: Orofaical region, sarcoma, soft tissue
How to cite this article:
Fomete B, Ogbeifun J O. Soft tissue sarcoma of the orofacial region: Our experience with 64 cases. Niger J Surg Res 2015;16:3-10 |
| Introduction | |  |
Soft tissue sarcomas (STSs) are solid malignancies mostly of mesodermal origin whose rarity and variety present formidable challenges in characterization and treatment. According to Pisters and Brennan, STS make up <1% of all oral malignancies. Like other tumors, they can occur at any anatomical site and at any age.[1] The extremities and trunk are favored sites for occurrence and only about 5–10% of STS occur in the head and neck region.[1],[2]
Soft tissue sarcoma have varied cell origin, but all STS are considered as a group because of the similarities in their clinical features, natural history, treatment, and disease outcome.[3]
Soft tissue sarcoma can range from relatively slow growth, causing little destructive growth, to being locally aggressive, regionally destructive, and having a great potential for systemic metastases.[2]
The age at presentation is variable with a mean of 50–55 years (minimum is 3 months and the maximum is 89-year-old) and the male/female ratio is approximately 2:1, which varies depending on the review series.[2] Adults and children are affected and in most reports 80–90% are adults and 10–20% are children.[1]
The symptoms depend on location, but the most frequently reported symptoms are the following: Headache, nasal obstruction, dysphagia, hoarseness, and dyspnea. However, the majority of patients are asymptomatic.[2],[4] The most frequently reported involved sites include the following: The face, neck, scalp, nasopharynx, maxillary antrum, cranial base, and parotid gland.[2]
Rhabdomyosarcoma (RMS) is the most common histologic type of STS in the oral and maxillofacial region, followed by the malignant fibrous histiocytoma (MFH) and the fibrosarcoma,[1],[2],[3] and neurofibrosarcoma.[3]
Surgery is the primary modality of treatment. Radiotherapy is usually used as an adjuvant to achieve better local control. However, there are isolated case reports of use of radiotherapy as a primary modality.[4],[5]
The prognosis of STS depends upon such factors as histological malignancy grading, the size of the primary tumor, location of the tumor, development of metastases, margins for surgical procedures, as well as recurrence.[4]
Reports from Africa on the clinical behavior of oral and maxillofacial STS are scanty and are mostly short reports.[1] This study presents orofacial STSs in Zaria North West Nigeria.
| Patients and Methods | | |
Medical records of patients with histopathologically diagnosed malignant oral and maxillofacial tumors between January 2003 and December 2013 were retrospectively reviewed at the Maxillofacial Unit, Ahmadu Bello University Teaching Hospital, Zaria, and Nigeria. The unit is the oldest maxillofacial center for the management of orofacial diseases in Northern Nigeria. Patient records examined included case files operative records and histopathology results. Cases of STS were selected from other malignancies and analyzed for age at presentation, sex, tumor site, clinical features, histopathological type, treatment, and follow-up reports. Tumor staging and grading was not done routinely within the study period.
| Results | | |
Soft tissue sarcoma constituted 64 cases (5.5%) out of 1170 cases of tumor in the orofacial region.
There were more male than female in a ratio of 1.28:1. The age range was from 7 months to 70 years with a mean of 29.3 years and 37.8% being <20 and about 62.2% being above 20 years. RMS was the most common lesion (39%) followed by fibrosarcoma (15.6%), MFH (7.8%) [Table 1]. The most common site was the mandible (45%) followed by the cheek (25%), palate (16%), and maxilla (14%). Some patients had both mandible and cheek involved while other had both palate and maxilla involved. The most frequent mode of treatment was surgery followed by radio and chemotherapy. A few patients (about 7%) declined therapy.
| Discussion | | |
Many STS are of mesodermal tissue origin such as RMS, fibrosarcoma, and liposarcoma while a few are of neuroectodermal origin such as malignant schwannoma and Ewing's sarcoma (ES). STS of the head and neck are quite rare with only a few reports in English literature.[1],[3] Some case reports from Africa are on specific tumors. STS make up <1% of all malignancies in the head and neck region and between 5% and 10% of all body sarcomas.[1]
Soft tissue sarcoma was <1% (64 cases) of all malignancies of the oral and maxillofacial region confirming its frequently reported rarity although this was about 43% (26 cases) higher than previous report from same center.[1] Male predilection in this study was 56.2%. This is comparable with 51–66.7% by previous authors.[1],[2],[3],[6],[7],[8]
Though no age group is exempt from sarcomas, maxillofacial STS generally affect the younger age group less commonly.[1],[3] In this study, the youngest patient was 0.5 years and the oldest 74 years with a mean of 25.6 years. This was comparable with 28.5–43.1 years (24 days–92 years) by previous authors.[1],[3],[6],[7],[8] Between 80% and 90% of STS occur in adults while 10–20% of patients are children.
The most common type of STS differs in different reports. According to González-González et al.,[7] malignant peripheral nerve sheat tumor was the most common (17.6%) followed by RMS (13.7%). According to Adebayo et al.,[1] Greagar et al., observed that fibrosarcoma is the most common (27%) followed by malignant schwannoma (15%), while Weber et al., noted that RMS (18%) was more common followed by MFH and fibrosarcoma. In his review of the literature, Adebayo et al.[1] reported that of 164 adult STS by the earlier author, angiosarcoma (16%) was the most common followed by fibrosarcoma (12%) and unclassified sarcomas (11%). Pandey et al.[3] reviewing 22 adult patients from India found unclassified spindle cell sarcomas (32%) and MFH and RMS (14% each). Adebayo et al.[1] in his series involving 38 cases, the foremost STS were RMS and fibrosarcoma (26% each) and MFH and liposarcoma (13% each). Meanwhile, our series of 64 cases found RMS (39%) the most common followed by fibrosarcoma (15.6%) and MFH (7.8%). This shows that while fibrosarcoma has increased by 1.6%. RMS has seen an increase from 14% to 39% and MFH a decrease from 13% to 7.8% in our center. There is no reason we can advance to justify this. Our findings agree with Fasunla and Adekunle,[8] (RMS [44.4%]) and Salcedo-Hernández et al.[6] (17%).
Rhabdomyosarcoma is the neoplastic analogue of the embryogenesis of skeletal muscle. The rhabdomyoblast recapitulates skeletal muscle embryogenesis in a highly disorganized manner [1] and accounting for 40% of all sarcoma in the head and neck region.[2] The tumor appears to be the more common among Caucasians than Negroes causing speculation of a genetic predilection. The paucity of reports on head and neck RMS from Africa makes these conclusions tenuous.[1] Twenty-five cases of RMS seen in this study had a male to female ratio of 1:1.1 while Adebayo et al.[1] same center found 10 cases with a male to female ratio of 1.5:1. Among the 25 cases in this study, 23 had histological subtype available; 16 alveolar and six embryonale. These findings were contrary to Adebayo et al.,[1] from same center with more embryonal (5) subtype than alveolar (1), but agree with Fasunla and Adekunle [8] and González-González et al.,[7] who got more alveolar RMS (4 cases each) than embryonal (3 and 2 cases, respectively).
According to Gonzalez-Gonzalez et al.,[2] the site varies depending on the published series. According to Adebayo et al.,[1] the cheek was the most common site overall (40%) followed by the mandible (20%). In our study, we found the cheek (35%) most common site followed by cheek-mandible (30%) and the mandible (15%). This shows that the cheek remains the most common site in our center. Oral RMSs are classified within the nonorbital, nonparameningeal group of tumors, which present a better prognosis and tend not to invade the central nervous system.[2],[9],[10] Presenting features of oral and maxillofacial RMS was frequently as swelling (90%), pain (60%) while ulceration of skin or mucosa was uncommon (20%). According to Suresh et al.,[10] signs and symptoms depend on the primary site, seen as painless swelling, throat discomfort or nasal airway obstruction or may be diagnosed accidentally during clinical examination. The presenting symptoms for RMSs of the orofacial region include painful infiltrative growth of short duration, paresthesia, loss of teeth and trismus characterized by fast growth. Pain, proptosis, diplopia, strabismus, decreased hearing, nasal obstruction, dysphagia, cervical lymphadenopathy are other signs, and symptoms.
Pandey et al.,[3] reported 2 cases of RMS mimicking gingival epulis associated with spontaneous exfoliation of teeth. Histopathologic diagnosis is based on conventional light microscopy and confirmed by immunohistochemistry. Antibodies against desmin, muscle-specific action, and myoglobin are most widely used for diagnostic purposes.[2]
Four histologic varieties; pleomorphic, alveolar, embryonal and botryoid types have been described.[1],[2],[9],[10] Among these forms, the embryonal is reportedly more common in the maxillofacial region most commonly affecting the hard palate.[1] RMS embryonal and alveolar subtypes are the most common soft tissue malignancy of the head and neck in children, comprising approximately 5% of all childhood cancers and nearly 50% of STSs arising in children 0–14 years of age,[1],[2] while the pleomorphic type is almost exclusive in adult.[2],[10] In the younger adults, the tumor is more frequently found affecting the extremities and trunk. In 110 embryonal RMSs of the body, Enzinger and Shiraki found the lesion occurring between 10 and 20 years of age (mean age 15 years). From the 5 cases of embryonal subtype in their series, Adebayo et al.[1] found that all but one was below 10 years of age. In our series, 4 out of the 6 patients were below 10 years and one was 13 years.
Staging of RMS according to intergroup RMS study (IRS).
- Localized disease, tumor resected completely, regional lymph nodes not involved
- Localized disease with microscopic residual disease or regional disease with or without microscopic residual disease
- Incomplete resection with the gross residual disease
- Metastatic disease.[9]
Adebayo et al.[1] in his review of literature observed that the earlier author said a combination of surgery, radiation treatment, and multi chemotherapy could give dramatic survival rates in patients with RMS.[1]
The gold standard for treating RMS according to IRS-IV is complete surgical excision followed by chemotherapy with a combination of vincristine, actinomycin-D, and cyclophosphamide. Hematopoietic growth factors are given with the chemotherapy regimen and local radiation therapy is optional.[10]
Radiotherapy as the primary treatment has been reported with varying success, while adjunctive radiation therapy is given whenever a tumor is not completely surgically removed. Randomized trials on adult sarcoma in general found that the addition of radiation resulted in significant improvement in local control over surgery alone. However, RMSs in adults are not as radiosensitive as those in children.[2]
Pellitteri et al.[11] believe that while the influence of the size of head and neck STS on prognosis is controversial; the possibility of successful en bloc resection of tumor is limited in large tumors due to involvement of critical neurovascular structures. Hence, poor local control and survival would accompany surgical therapy of large lesions in the head and neck. During this study period, facilities for head and neck radiotherapy were not available within a 700 km radius of our center while the cost of radical surgery with need for reconstruction remains unaffordable to many of our patients unlike the Indian cases reported by Pandey et al. The current coverage of national health insurance is restricted to employees of governments.[12] Despite the gruesome sizes on presentation of many tumor cases in Nigeria, cases of default after diagnosis and inoperable cases abound. This is due to ignorance of medical problems among patients and their relatives, poor access to modern health care facilities, native superstitions forbidding surgical treatment and the social problem of poverty. Hence, the combination of ignorance, poverty, and inadequate medical infrastructure limit treatment options and survival of STS patients in our environment.[1],[12] The impact of treatment on survival of the cases seen in this report could not be assessed, as follow-up review visits was poor in this study.
Prognosis depends on site of the tumor, tumor stage, histological subtype, and age of the patient. Patients below 1-year have the worst prognosis with a 3 years estimated failure-free survival rate of 55% compared to 83% in 1–9 years age group and 68% in those ages 10 or older and suggested 83% survival rate for embryonal subtype and lower survival for other subtypes.[10] The 5- survival rate is approximately 85% for this RMS subtype.[2]
Rhabdomyosarcomas are associated with high rates of recurrence and distant metastases through lymphatic and hematogenous spread to lungs, lymph nodes, and bone marrow followed by heart, brain, meninges, pancreas, liver, and kidney.[9]
Fibrosarcoma is defined as a malignant spindle cell tumor that shows a herringbone or interlacing fascicular pattern without the expression of other connective tissue cell markers. Fibrosarcoma can arise in soft tissues or within bones. Intraosseous fibrosarcomas may develop enosteally or possibly periosteally, affecting the bone by spreading from adjacent soft tissue.[2] Fibrosarcomas can occur in any location, but the bone extremities are the main affected sites; occurrence in the maxilla is rare, with an incidence ranging from 0% to 6.1% of all primary fibrosarcomas of the bone. The mandible is the most common site for fibrosarcomas. Adebayo et al.[1] in his review of literature observed that 45% of fibrosarcomas occur between the ages of 20 and 40 years while Dahlin and Ivins found 13 of 114 central bone cases of the lesion originating in the mandible. Adebayo et al.[1] from our center found 10 cases of fibrosarcoma occurred between 8 and 60 years of age with 70% below the age of 40 years. We found 10 cases as Adebayo et al.[1] occurring between 0.5 and 50 years of age with 66.6% below the age of 40 years. Among their cases, the mandible was the most common site (60%) followed by the palate (20%).
The clinical behavior of fibrosarcoma is characterized by a high local recurrence rate and a low incidence of locoregional lymph node and/or distant hematogenous metastases.[2] Fibrosarcoma grows rapidly or slowly.[1]
The histological appearance of fibrosarcoma does not allow a distinction between a tumors of the bone from one arising in soft tissue. Histologically, the degree of differentiation is variable, from being comparable to a benign fibroma to a highly anaplastic tumor, thus presenting a diagnostic dilemma to histopathologists. Fibrosarcoma can be graded as either a low or high grade of malignancy.[2] The histological appearance of high grade fibrosarcoma may be similar to other tumors, such as MFH, liposarcoma or synovial sarcoma. The positive immunostaining for vimentin, together with negative staining for muscular immunomarkers, helps to diagnose fibrosarcoma.[2]
The most acceptable form of treatment for fibrosarcoma is radical resection. Any form of limited excision especially due to its pseudo encapsulation inevitably leads to recurrence.[1],[13]
No survivor was recorded 5-year after treatment of fibrosarcoma of the jaws in the Netherlands.[1]
Liposarcoma is the second most common STS in adults. Its occurrence in the head and neck region is reported to be very rare. The majority of liposarcomas occur in middle-aged adults; however, very uncommon cases of liposarcoma can be generated in infancy and early childhood. The occurrence of liposarcoma in the head and neck region is rare, comprising 5.6–9% of all cases Gonzalez-Gonzalez et al.[2] Liposarcoma of the oral cavity is even less frequent, making up about 10% of all cases in the head and neck.[2] As with liposarcomas elsewhere in the body, most cases present in adults, and there is a male predominance. Factors considered to be important in the etiology of liposarcomas include genetics, trauma and irradiation.[2]
Even though fat tissue is abundant in the oral and maxillofacial region, liposarcoma in this region is exceptionally rare. Between 1958 and 1965, only 4 cases were seen in Southern England. In his review of the literature, Adebayo et al.[1] noted that the first case of liposarcoma from our center in 1978. This tumor is rare below the age of 30 years and shows a slight male preponderance (55%) according to Enzinger and Winslow.[1] Adebayo et al.[1] from our center reported that 80% of the cases in their study where above 30-year-old while the male to female ratio was 1.5:1. In this study, we have only 1 case of liposarcoma and it is a female of 50 years. This shows again its rarity.
Liposarcoma occurred mostly as cheek swellings (60%), the rest were in the palate (20%) and maxilla (20%). The only case we present here occurred in the cheek. Several histological sub classifications of liposarcoma have been described. One classification describes the cell types as myxoid, round cell, adult, and pleomorphic. It has been noted that majority (71% of 35 cases) of liposarcomas of the maxillofacial area are of the myxoid cell type, are well differentiated with a good prognosis. Among the cases by Adebayo et al.,[1] 60% were of the myxoid variety. Our case was a dedifferentiated type. Radiological investigations are necessary in most cases to determine precise size, localization, limits, extensions of the tumor, and its relations with neurovascular structures. It is also necessary for detecting distant metastases.[2]
Liposarcoma appears to have a clear capsule and is easy to separate, but it often infiltrates the surrounding structures microscopically, so occasionally, incomplete resection occurs.[2]
Surgical excision with or without radiotherapy is used for treating liposarcoma with prognosis related to several factors especially tumor cell type. The case we had was inoperable and referred for radiotherapy and chemotherapy while Adebayo et al.,[1] treated 4 cases two by surgery, one chemotherapy, and one radiotherapy.
Malignant fibrous histiocytoma was first described by Ozzelo et al., in 1963 and by O'Brien and Stout in 1964. It was widely accepted as a clinicopathological entity after the description of cases by Kempson and Kyriakos in 1972.[2] The etiology is unknown, and the histogenesis remains controversial. Several hypotheses have been suggested, including an origin from true histiocytes, fibroblasts, both fibroblasts and histiocytes, or from primitive mesenchymal cells.[2] MFH is now recognized as one of the most common STSs in adults. In addition to occurring in soft tissue, it can also occur as a primary intraosseous tumor in bones. It affects, in order of frequency, the lower extremity, the upper extremity, the retroperitoneum and abdominal cavity, and lastly, the head and neck, where it accounts for 1–3% of all cases. Therefore, it is relatively uncommon in the head and neck region.[2]
Malignant fibrous histiocytoma is regarded as one of the most common STS of later life where it affects the musculature of the limbs. It is rare in the maxillofacial region. In a large series of 200 cases, Blitzer et al., found only six in the head and neck. According to Pandey et al.,[3] all 3 cases of MFH from a Regional Cancer Center in India occurred between 13 and 54 years of age, all are males. According to Adebayo et al.,[1] 80% of cases of MFH were above the third decade of life, (mean age 39.4 years). [Table 2] shows that 80% of cases seen here were above 30 years with a mean of 55.6 years. Of all the 5 cases, 60% were male and 40% female while Adebayo et al.[1] same center got all males (5 cases). This further raises the possibility of male predilection for occurrence. The tumor is believed to occur mostly in the sixth decade of life The tumor is rare in the oral soft tissues; most are central lesions of the jawbones. Ialez et al., on the report by Pandey et al.,[3] 66% of cases of MFH were in the jawbones. 4 of the 5 cases in Adebayo et al.[1] series occurred at the jawbones similar to the findings of Pandey et al. Meanwhile we had 2 cases on the mandible, 1 case in the maxilla, frontal region, and cheek each.
Histologically, the tumor contains both fibroblast-like and histiocyte-like cells in varying proportions, with spindle and round cells exhibiting a storiform arrangement. These tumors have been divided into four morphologic subtypes that depend on the predominant cellular components: Storiform – pleomorphic (50–60%), myxoid (25%), giant cell (5–10%), and inflammatory (about 5%).[2]
Radical local excision is the most useful form of treatment for this lesion.[1],[13] This was also used in this study.
Malignant schwannoma can occur de novo or less frequently from preexisting lesions of neurofibromatosis. While cases occurring de novo present later in life, those arising secondarily are generally seen in adolescents and young adults.[1] Their report had no history of malignant schwannoma arising secondarily and there were males aged 46–48 years. In this report, all our cases were also male with the age range between 25 and 37 years and a mean of 31.25 years. Any of the oral soft tissues such as the lip, palate, gingiva or the hard tissues such as the jawbones can be involved in the lesion.[1] Patients managed in this report presented with swelling, pain and ulceration of the palate and nostril. Prognosis of malignant schwannoma varies greatly and factors responsible are tumor location, degree of differentiation, duration at presentation, and method of treatment. Tumors secondary to von Recklinghausen's disease have a worse outcome compared to primary tumors. Recurrence following local excision can be up to 80% with a 5-year survival between 15% and 30%.[1]
Leiomyosarcoma usually occurs in the soft tissues of the extremities and trunk; only 3% of leiomyosarcomas are in the head and neck. In the head and neck region, most leiomyosarcomas occur in the nasal cavity and paranasal sinuses, mouth, and larynx.[2] The scarcity of the smooth muscle in the head and neck region may be the probable reason for the rarity of leiomyosarcoma.[2] This report got 2 cases all male with ages 45 and 65 years of life (mean age 55 years). Adebayo et al.[1] got an onset of 39–65 years (mean age, 55.4 years).
The signs and symptoms of leiomyosarcoma involving the head and neck region depend on the site and the size of the tumor. Hoarseness, stridor, dyspnea and dysphagia are the most common complaints of the laryngeal and the parapharyngeal tumors. While the initial symptom in a patient with laryngeal leiomyosarcoma in one report was dysphonia, the main symptom in a second patient with parapharyngeal leiomyosarcoma was dysphagia due to the mechanic compression of the cervical esophagus.[2] The lack of any distinguishing clinical features and the rarity of these lesions often result in their being mistaken for the more common lesions affecting the oral cavity, and correct diagnosis is made only following definitive histological examination.[2] Histopathologically displayed a prominent spindle cell component, with the cells arranged in intersecting fascicles, containing characteristic “cigar-shaped” nuclei.[2] In most instances, immunohistochemistry may provide useful clues to the diagnosis; muscle-specific markers for smooth muscle actin and vimentin are most frequently detectable, but myofibroblastic tumor cells, RMS and inconstantly, spindle cell carcinomas may display a similar immunoprofile.[2] Although numerous prognostic factors, including size, site, grade, and TNM stage, have been identified for leiomyosarcoma arising in other sites, there are no reliable prognostic factors in the case of primary oral leiomyosarcoma.[2]
Angiosarcoma is a malignant neoplasm that frequently occurs in the skin and subcutis or in a visceral location and very rarely affects the oral cavity representing 1% of all STSs.[2],[14] Clinically, angiosarcoma appears as painful, spontaneously bleeding poorly demarcated round or ovoid nodular tumor that is, red-blue to purplish in color.[2],[14] Angiosarcomas of the head and neck most commonly involve the scalp, and only 4–5% of them form in the pharynx, oral cavity or maxillary sinus.[2] They may represent either primary or metastatic lesions. In a recent review of the literature, only 35 cases have been reported.[3] This report had 2 cases all males with their ages being 30 and 40 years. There are only a few articles in the literature that discuss patients with angiosarcoma, but most of these angiosarcomas affected the irradiated region or originated in the skin and secondarily affected the parotid gland. All angiosarcomas tend to be aggressive, and they are often multicentered.[2]
Angiosarcomas predominantly affect elderly men and may be present in any region of the body, but they usually occur in the skin or superficial soft tissues (head and neck) in the postradiotherapy area. The prognosis is poor because of frequent local recurrence and metastatic spread to the lymph nodes, bones (vertebrae), and lungs.[2] These tumors have a high local recurrence rate and metastasize because of their intrinsic biological properties and because they are often misdiagnosed, which leads to a poor prognosis and high mortality rate.[2] Their clinical outcomes are poor due to a rapid growth and high risk of metastatic extension.[2] The microscopic appearance of angiosarcoma varies from epithelioid to spindled areas, with the former being more common. Various prognostic factors have been reported, including older age, tumor size larger than 5 cm, high grade, positive margin, and lymphedema field location.[2] Magnetic resonance imaging (MRI) and contrast-enhanced computed tomography are nonspecific for diagnosis, but they may be used to define the extent of the primary tumor and evaluate distant metastasis. The diagnosis of angiosarcoma can only be established by microscopic examination.[2] Treatment of angiosarcomas is greatly complicated by the diffuse infiltration typical of these tumors.[2]
Recurrence after local treatment manifests primarily in local failure, yet distant metastasis is not insignificant in the posttreatment failure group. These factors, both for local and distant spread, are reflective of the highly aggressive nature of this illness and serve to explain the poor survival statistics.[2]
Ewing's sarcoma is an unusual disease comprising about 4–6% of all primary bone tumors. It originates in the marrow cavity and is found in the epiphyses of long and flat bones. Involvement of the head and neck in ES is very unusual, accounting for approximately 1–4% of cases. The skull and mandible are the most frequent sites. The mandible is more affected than the maxilla.[15],[16] It is rare after the third decade and occurs most often in the second decade. It is more common in males than females.[17] This study present 2 cases both within the range of 10–20 years with a mean of 16 years and all being male. This mean and age range is in agreement with Lopes et al.[18] and Fonseca et al.[17] Symptoms and signs are those of slow growing, firm, enlarging mass with or without pain or tenderness. Some cases present with systemic symptoms such as fever. Oral symptoms could include swelling, loosening of the teeth and paresthesia.[16]
According to Lopes et al.,[18] MRI is widely accepted as the image method of choice for evaluation of the extend of the primary lesion and its relationship with anatomic structures such as glands and muscles. Several studies have demonstrated the usefulness of scintigraphy for diagnosis, control, and detection of skeletal metastasis of ES.
Due to the high local reoccurrence rate (20%) following radiation therapy alone, radical surgical removal must be attempted to increase local control whenever feasible. The same applies to the mandible, since today's reconstruction techniques alleviate esthetical and functional impairment to the patient. Radiotherapy must be used as neoadjuvant therapy or in nonresectable primary radiosensitive tumors. Chemotherapy must be reserved to prevention and treatment of metastasis.[17] The appropriate treatment for ES has been the surgical excision of the tumor associated with radiotherapy and chemotherapy.
The association of surgery, radiotherapy, and chemotherapy has significantly improved the 5-year survival ratio, now reaching 40–75%. The single most important indicator is the primary site, and thus, primary tumors of the head and neck, especially the mandible, have a significantly higher survival ratio. An extremely high erythrocyte sedimentation rate has been associated with a poorer prognosis. Death is usually due to disseminated hematogenic spreading of the disease.[17]
| Conclusion | | |
Soft tissue sarcoma remains a challenge in our center due to late presentation and affordability of treatment by our patients. Another contributing factor is the believe that cancer cannot be treated with orthodox medicine.
From the last report, we noted about 43% increase in cases of STS in our center.
| References | | |
| 1. | Adebayo ET, Ajike SO, Adebola A, Adekeye EO. Oral and maxillo-facial soft tissue sarcomas in an Africa population. Niger J Surg Res 2006;8:135-9.  |
| 2. | |
| 3. | Pandey M, Chandramohan K, Thomas G, Mathew A, Sebastian P, Somanathan T, et al. Soft tissue sarcoma of the head and neck region in adults. Int J Oral Maxillofac Surg 2003;32:43-8. |
| 4. | Markowski J, Dziubdziela W, Podlejska K, Likus W, Pasternak K, Kajor M, et al. Soft tissues sarcomas of the head and neck in adult: Histo-clinical analysis of 30-years material in the data of ENT Department of Silesian Medical University. Otolaryngol Pol 2012;66:382-6. |
| 5. | Ketabchi A, Kalavrezos N, Newman L. Sarcomas of the head and neck: A 10-year retrospective of 25 patients to evaluate treatment modalities, function and survival. Br J Oral Maxillofac Surg 2011;49:116-20. |
| 6. | Salcedo-Hernández RA, Lino-Silva LS, Mosqueda-Taylor A, Luna-Ortiz K. Soft tissue sarcomas of the head and neck. Clinical and pathological evaluation of 108 cases in Mexico. J Craniomaxillofac Surg 2014;42:1566-71. |
| 7. | González-González R, Bologna-Molina R, Molina-Frechero N, Domínguez-Malagon HR. Prognostic factors and treatment strategies for adult head and neck soft tissue sarcoma. Int J Oral Maxillofac Surg 2012;41:569-75. |
| 8. | Fasunla AJ, Adekunle D. Retrospective review of soft tissue sarcoma of the head and Neck in a West African Hospital. Alex J Med 2013;49:43-8. |
| 9. | Konidena A, Kode M. Intraoral rhabdomyosarcoma in a young boy. JIAOMR 2010;22:s73-5. |
| 10. | Suresh D, Manjula M, Kumuda P, Aruna P. Embryonal rhabdomyosarcoma of the oral cavity – A case report. J Res Adv Dent 2013;2:78-81. |
| 11. | Pellitteri PK, Ferlito A, Bradley PJ, Shaha AR, Rinaldo A. Management of sarcomas of the head and neck in adults. Oral Oncol 2003;39:2-12. |
| 12. | Fomete B, Adebayo ET, Agbara R, Ayuba GI. Massive peripheral myxoma in a child: Case report and review of the literature. J Oral Maxillofac Surg Med Pathol 2014;26:163-5. |
| 13. | Fernandez Sanroman J, Alonso del Hoyo JR, Diaz FJ, Gil-Diez JL, Monje F, Naval L, et al. Sarcomas of the head and neck. Br J Oral Maxillofac Surg 1992;30:115-8. |
| 14. | Nagata M, Yoshitake Y, Nakayama H, Yoshida R, Kawahara K, Nakagawa Y, et al. Angiosarcoma of the oral cavity: A clinicopathological study and a review of the literature. Int J Oral Maxillofac Surg 2014;43:917-23. |
| 15. | Pitak-Arnnop P, Bellefqih S, Bertolus C, Chaine A, Dhanuthai K, Gruffaz F, et al. Ewing's sarcoma of jaw bones in adult patients: 10-year experiences in a Paris university hospital. J Craniomaxillofac Surg 2008;36:450-5. |
| 16. | Ko E, Brouns ER, Korones DN, Pochal WF, Philipone EM, Zegarelli DJ, et al. Primary Ewing sarcoma of the anterior mandible localized to the midline. Oral Surg Oral Med Oral Pathol Oral Radiol 2013;115:e46-50. |
| 17. | Fonseca AS, Mezzalira R, Crespo AN, Bortoleto AE Jr, Paschoal JR. Ewing's sarcoma of the head and neck. Sao Paulo Med J 2000;118:198-200. |
| 18. | Lopes SL, Almeida SM, Costa AL, Zanardi VA, Cendes F. Imaging findings of Ewing's sarcoma in the mandible. J Oral Sci 2007;49:167-71. |
[Table 1], [Table 2]
|









 Search Pubmed for
Search Pubmed for