|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 16
| Issue : 1 | Page : 11-14 |
|
Limb amputations in Nigeria: The National hospital abuja experience
Habila Umaru, Chukwuemeka Christian Madubueze, Abdulrazak Alada, Chibuike Mathias Onu
Department of Surgery, Orthopaedic Unit, National Hospital, Abuja, PMB 425, Garki-Abuja, Federal Capital Territory, Nigeria
| Date of Web Publication | 8-Oct-2015 |
Correspondence Address:
Habila Umaru
Department of Surgery, Orthopaedic Unit, National Hospital, Abuja, PMB 425, Garki-Abuja, Federal Capital Territory
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/1595-1103.166884

Background: Limb amputation is a common live saving surgical procedure in orthopedics and trauma practice that is associated with profound psychological, social and economic consequences on patients and his family. Current reports from some parts of Nigeria suggest that diabetic complications are taking the lead as cause for limb amputations in place of trauma the traditionally known etiological factor in the country.
Objectives: To review the indications for amputations in our center and to compare our findings with published information, in view of its effect on the individual and the society and to suggest preventive measures.
Materials and Methods: An 8 years retrospective study of extremity amputations performed in our hospital. Data on age, gender, indication for amputation, level of amputation, and outcome of surgery were extracted from the patients' case files and the operation register. Data were analyzed using SPSS version 16 and result presented in diagrammatic and tabular form.
Results: The records of 106 patients were analyzed, there were 73 males and 33 females (ratio of 2.2:1), the age ranged from 8 to 92 years with a mean age and (standard deviation) 43.76 (±18.69) years. Diabetic foot gangrene was the most common indication for limb amputation in 46 (43.3%) patients compared to trauma 22 (20.8%). Below knee amputation was the most frequent level of amputation 50 (47.2%). The most frequent complication encountered was surgical site infection in 30 (28.3%).
Conclusion: Diabetic foot gangrene was the leading indication for amputation in this study. Intense public enlightenment on prevention, early detection and effective treatment of diabetes and its complications will reduce the incidence of amputations in our environment. Keywords: Amputation, diabetic foot, indications, limb
How to cite this article:
Umaru H, Madubueze CC, Alada A, Onu CM. Limb amputations in Nigeria: The National hospital abuja experience. Niger J Surg Res 2015;16:11-4 |
| Introduction | |  |
Limb amputation is an ancient surgical procedure that has retains its relevance in modern time,[1] the procedure has been practiced for punitive, ritual and therapeutic reasons including trauma, peripheral vascular disease (PVD), tumor, infection and congenital anomalies.[2],[3],[4],[5] The decision to amputate a patient's limb is often one of the most difficult ones for the surgical team to make and a most trying period for the patient and his relations to give consent for the procedure.[6] The anxiety of persons undergoing this procedure is rooted on the premise that major limb amputations are essentially disfiguring operations that carry a fairly high perioperative mortality and morbidity and persons who have undergone amputations are often viewed as incomplete individuals.[2],[6],[7]
The indications of limb amputations vary from place to place, whereas in developed countries PVD ranks first as cause for amputation,[8] in developing countries trauma, infections, uncontrolled diabetes mellitus (DM) and malignancies are some of the published leading causes for amputation.[2],[9]
In Nigeria, the reported leading indication over the years has been trauma while traditional bone setters' (TBS) gangrene with malignancy and diabetic gangrene trailing as rear guards.[3],[9],[10],[11],[12] However, recent data emanating from different parts of the country is suggesting otherwise, singling out diabetic foot gangrene as a leading cause of amputation in many centers.[6],[13] Other authors have also drawn public attention to the increasing importance of diabetic limb lesions in Nigeria.[14],[15],[16] The reversal may not be surprising in view of enlightenment programs in the last decade on the problems of TBS and the advantage of early hospital presentation in trauma cases,[13] which might be yielding attitudinal change.
| Materials and Methods | | |
This is a retrospective study of extremity amputations performed in our hospital between January 2005 and December 2013. A total of 126 patients had 128 limb amputations within the period, only 106 were entered for the study, 20 of the patients were excluded due to inadequate information in their records. Data on age, gender, indication for amputation, level of amputation, and outcome of surgery were extracted from the patients' case files and operation register. Data were analyzed using the Statistical Package for Social Sciences (SPSS) version 16 (Chicago, SPSS Inc.) and result presented in diagrammatic and tabular form.
| Results | | |
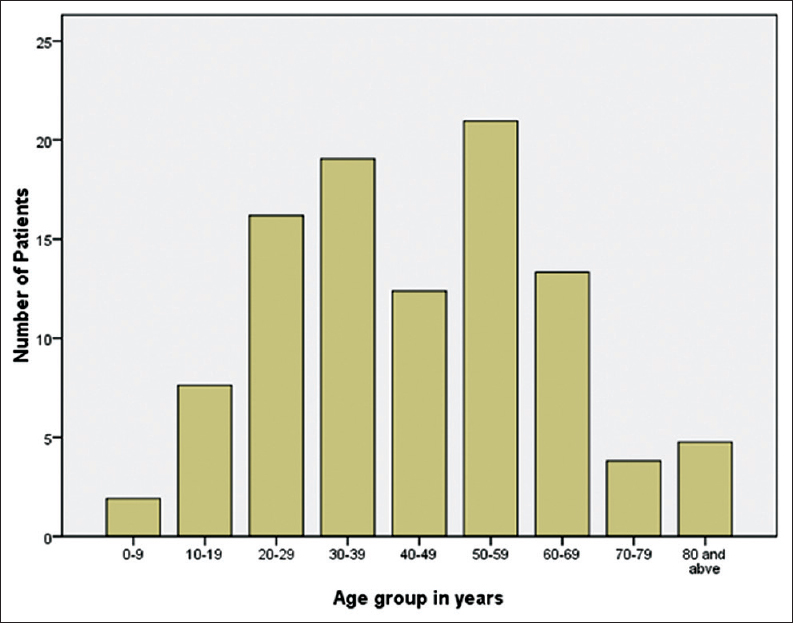
The records of 106 patients were analyzed, and there were 73 male and 33 female with a ratio of (2.2:1), the age ranged from 8 to 92 years (mean 43.76 &± 18.69). More than 60% of cases of amputations were between the ages of 20 and 59 years. There was biphasic peak age of occurrence of amputations at 30–39 years and 50–59 years as shown in [Figure 1].
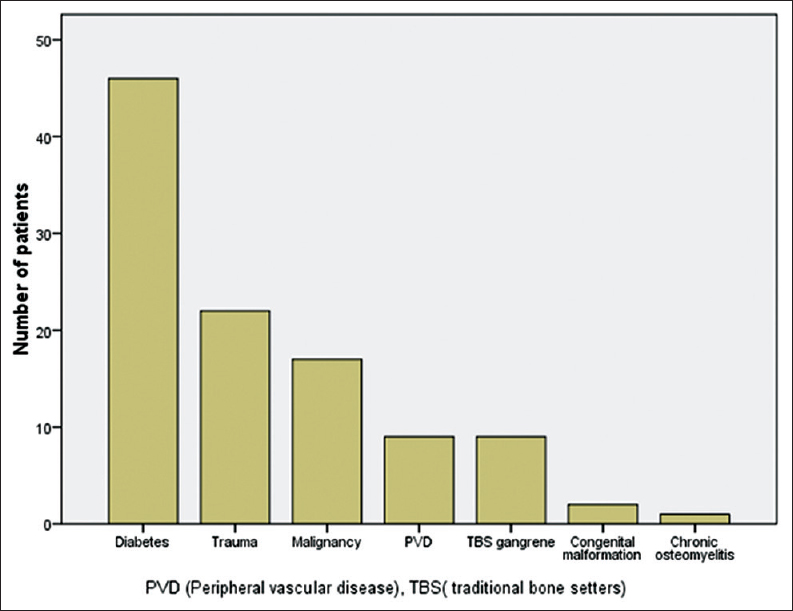
Diabetic foot gangrene was the most common indication for limb amputation in 46 (43.3%) patients while trauma accounted for 22 (20.8%), the rest of indications are as shown in [Figure 2].
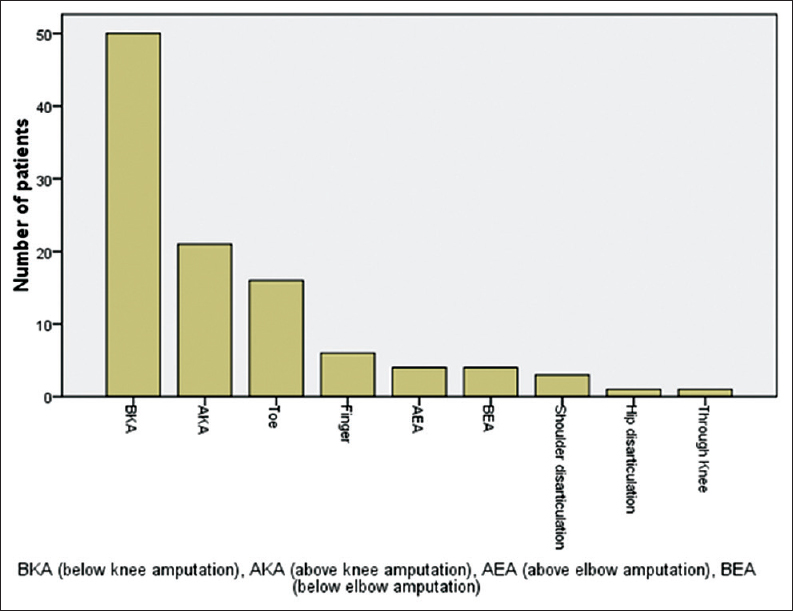
There were 89 (83.9%) amputations involving the lower limb, of these number, DM was the cause for amputation 45 (42.5%) cases, while there were 17 (16.1%) upper limbs amputations out of which trauma was the reason for the procedure in 13 (12.3%) patients. Below knee amputation (BKA) was the most frequent level of amputation that accounted for 50 (47.2%) of cases.
The details of other levels of amputation are as shown in [Figure 3].
The most frequent complications encountered were surgical site infection in 30 (28.3%) patients, wound dehiscence 13 (12.3%) and reamputations due to ascending gangrene in 8 (7.5%) cases. We recorded a total of 13 (12.3%) mortality. Of them, 11 (84.6%) of the total deaths were complications of diabetes while the rest (15.4%) were due to complications of advanced malignant tumors.
| Discussions | | |
Amputation is a common procedure in orthopedics and trauma practice for therapeutic reasons, usually to save patient's life.[15] However, it is often associated with profound economic, social and psychological effects on patient and their family.[2] This is partly due to unavailable or unaffordable rehabilitation facilities in most of our hospital setting,[17] thereby making their reintegration to the society much more difficult or impossible. Hence, the need for regular review of the indications of this procedure to identify trends and proffer appropriate preventive measures.
The male preponderance in this study is consistent with findings in other published series,[3],[13],[15],[16],[17] but a closer analysis of male to female ratio of 2.1:1 is much lower than finding of Ajibade et al.[1] in Jawaid et al.[18] in Pakistan who reported male to female ratio of 6.7:1 and 6.6:1 respectively, they observed that the male to female ratio is higher when trauma is the predominant indication for amputation compared to diabetic gangrene and PVD. This may explain the low male: female ratio in this survey, the predominant indication being diabetic foot gangrene.
The peak age of incidence is observed in the sixth decades, as seen in this study is comparable to recent report from South-West,[13] South-South [6] Nigeria and North-Western Tanzania [2] who reported similar age incidence. A common factor to these recent reports is the fact that diabetic foot was the leading indication for amputation in all of them. However, it is at variance to earlier reports from Nigeria,[1],[3],[16] which indicated the peak age incidence of amputation in the third and fourth decades. The significant difference in age of incidence as observed in these studies is due to variation of the indications for amputation, with trauma as the commonest reason for amputation in the younger age group, compared to diabetic foot gangrene and PVDs in the elderly.[6],[13]
This study agreed with the documented triad of diabetic gangrene, trauma and malignancy as responsible for most amputations in Nigeria to a variable extent [Figure 2].[17] Our findings also buttress the observations from other parts of the country, pointing out that diabetic foot gangrene has overtaken other causes as the leading indication for limb amputations in our environment.[12],[14] These also corroborate the recent report highlighted by Dada and Awoyomi and reechoed by Odatuwa-Omagbemi and Adiki of the changing trend of indications of limb amputation in Nigeria from trauma and TBS gangrene to diabetic foot disorders.[6],[13] The increased incidence of diabetic foot complications requiring lower limb amputation may reflect the level of ineffectiveness of the early detection of DM and the foot at risk, medical education, patient compliance and overall control of DM in this population.[2]
On the other hand, the relative decline in trauma as a leading cause of amputation might be attributed to the recent ban on the commercial use of motorcycle (a major cause of pedestrian injuries and road crashes [19],[20]) in most major cities and townships in Nigeria.
In contradistinction, TBS gangrene, which featured prominently as an indication of amputation in Northern and South-Eastern Nigeria in many reports previously,[3],[12],[16],[17],[21] did not play significant role as reasons for amputation in this review. Some of the reasons adduced to current reduction in TBS gangrene are ascribed to possible change in attitude among the populace with increasing awareness of the problems of TBS and the advantage of early presentation in hospital following injury, which has been emphasized in previous reports.[2],[3],[13]
In agreement with other studies,[1],[6],[13],[16] most of our amputations were performed in the lower limbs and BKA was the most common type of amputation. Our finding is in conformity with other reports that lower extremities are injured more often than the upper extremities, and diabetic gangrene is commoner on the lower extremities than elsewhere on the body.[5],[6],[17]
However, at variance is an earlier report from Maiduguri, North-Eastern Nigeria and others that reported above knee amputation as the most common procedure performed than BKA.[2],[3],[17] Late presentation of trauma with ascending gangrene and complications of TBS, advanced diabetic foot gangrene or malignant lesions that have involved the underlying bones are identified factors that often force the surgeon to opt for a higher level of amputation.[2],[17],[21],[22],[23]
We observed wound infection rates of 28.3%, with close to half of them requiring secondary wound closure, this is comparable to report of 30% and 31.4% wound infection rates observed in Warri, South-South and Lagos, South-West of Nigeria respectively.[6],[13] Our reamputation rate of 7.5% (8 patients) is comparable to reports of 7.4% in Jos Nigeria, and 9.9% reported in Tanzania, but lower compared to 23% reported by Essoh et al.[24] in Coted'Ivoire.
Reasons alluded to variations in reamputation rates range from late presentation with advanced disease to the majority of amputations being relegated to junior doctors who has little experience thus, increases the chances of revision amputation.[2],[17]
We recorded a total of 13 (12.3%) mortality; this is similar to several reports of other authors [2],[16],[17] but higher than mortality of 7.0% reported from Warri, South-South Nigeria.[6] The mortalities in our study were diabetes-related complications, wound sepsis and advanced malignancies with metastasis, which is similar to the Tanzanian experience.[2]
| Conclusion | | |
Complications of diabetic foot ulcers were the most common risk factors for limb amputations in this study. Rigorous enlightenment of diabetic patients on foot care, effective treatment of diabetes and early detection/presentation of diabetes foot complications in hospitals will reduce the incidence of limb amputations in our environment.
| References | | |
| 1. | Ajibade A, Akinniyi OT, Okoye CS. Indications and complications of major limb amputations in Kano, Nigeria. Ghana Med J 2013;47:185-8.  |
| 2. | Chalya PL, Mabula JB, Dass RM, Ngayomela IH, Chandika AB, Mbelenge N, et al. Major limb amputations: A tertiary hospital experience in Northwestern Tanzania. J Orthop Surg Res 2012;7:18. |
| 3. | Umaru H, Gali BM, Ali N. Role of inappropriate traditional splintage in limb amputation in Maiduguri, Nigeria. Ann Afr Med 2004;3:138-40. |
| 4. | Magee R. Amputation through the ages: The oldest major surgical operation. Aust N Z J Surg 1998;68:675-8. |
| 5. | Olaolorun DA. Amputations in general practice. Niger Postgrad Med J 2001;8:133-5. |
| 6. | Odatuwa-Omagbemi D, Adiki O. Extremity amputations in Warri, South-South Nigeria. J West Afr Coll Surg 2012;2:14-24. |
| 7. | Masood J, Irfan A, Ghulam M. Current indications for major lower limb amputation. Pak J Surg 2008;24:228-32. |
| 8. | Abou-Zamzam AM Jr, Teruya TH, Killeen JD, Ballard JL. Major lower extremity amputation in an academic vascular center. Ann Vasc Surg 2003;17:86-90. |
| 9. | Olasinde AA, Oginni LM, Bankole JO, Adegbehingbe OO, Oluwadiya KS. Indications for amputations in Ile-Ife, Nigeria. Niger J Med 2002;11:118-21. |
| 10. | Thanni LO, Tade AO. Extremity amputation in Nigeria – A review of indications and mortality. Surgeon 2007;5:213-7. |
| 11. | Solagberu BA. The scope of amputations in a Nigerian teaching hospital. Afr J Med Med Sci 2001;30:225-7. |
| 12. | Ogunlade SO, Alonge TO, Omololu AB, Gana JY, Salawu SA. Major limb amputation in Ibadan. Afr J Med Med Sci 2002;31:333-6. |
| 13. | Dada AA, Awoyomi BO. Is the trend of amputation in Nigeria changing? A review of 51 consecutives cases seen at Federal Medical Centre Ebute Metta, Lagos, Nigeria. Niger Med J 2010;51:167-9.  |
| 14. | Solagberu BA. Diabetic foot in Nigeria – A review article. Afr J Med Med Sci 2003;32:111-8. |
| 15. | Teichmann J, Sabo D. Epidemiology and classification of diabetic foot syndrome. Orthopade 2009;38:1139-48. |
| 16. | Ofiaeli RO. Indications, levels and outcome of lower extremity amputations in Nnewi, Nigeria. J Med Invest Pract 2001;2:18-21. |
| 17. | Kidmas AT, Nwadiaro CH, Igun GO. Lower limb amputation in Jos, Nigeria. East Afr Med J 2004;81:427-9. |
| 18. | Jawaid M, Ali I, Kaimkanni GM. Current indications for lower limb amputations at civil hospital, Karachi, Pakistan. J Surg 2008;24:228-31. |
| 19. | Umaru H, Ahidjo A, Dogo H. Pedestrian injuries resulting from road traffic accidents: The Azare experience. Niger J Med 2007;16:169-72. |
| 20. | Falope IA. Motorcycle accidents in Nigeria. A new group at risk. West Afr J Med 1991;10:187-9. |
| 21. | Garba ES, Deshi PJ, Ihejirika KE. The role of traditional bone setters in limb amputation in Zaria. Niger J Surg Res 1999;1:21-4. |
| 22. | Holcombe C, Hassan S. Major limb amputation in Northern Nigeria. Br J Surg 1991;78:885-6. |
| 23. | Chalya PL, Mabula JB, Dass RM, Kabangila R, Jaka H, McHembe MD, et al. Surgical management of Diabetic foot ulcers: A Tanzanian university teaching hospital experience. BMC Res Notes 2011;4:365. |
| 24. | Essoh JB, Bamba I, Dje Bi Dje V, Traore A, Lambin Y. Limb amputations in adults in an Ivorian teaching hospital. Niger J Orthop Trauma 2007;6:61-3. |
[Figure 1], [Figure 2], [Figure 3]
|









 Search Pubmed for
Search Pubmed for