|
 
 |
| CASE REPORT |
|
| Year : 2016 | Volume
: 17
| Issue : 1 | Page : 14-16 |
|
Epithelioid hemangioma mimicking multinodular goiter: A case report and the review of the literature
Nasiru Abubakar1, Yawale Ilyasu1, Modupeola Omotara Samaila1, Aliyu U Bappa1, Karo C Akpobi1, Musa T Samdi2
1 Department of Pathology, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria
2 National Ear Care Centre, Kaduna, Nigeria
| Date of Web Publication | 16-May-2016 |
Correspondence Address:
Nasiru Abubakar
Department of Pathology, Ahmadu Bello University Teaching Hospital, Zaria
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/1595-1103.182475

Epithelioid hemangioma (EH) is an uncommon cutaneous vascular lesion often localized to the superficial dermis. We report a 55-year-old female with multilobular anterolateral neck mass which was clinically diagnosed as multinodular goiter. However, tissue histology revealed EH. Keywords: Epithelioid, goiter, hemangioma, multinodular
How to cite this article:
Abubakar N, Ilyasu Y, Samaila MO, Bappa AU, Akpobi KC, Samdi MT. Epithelioid hemangioma mimicking multinodular goiter: A case report and the review of the literature. Niger J Surg Res 2016;17:14-6 |
How to cite this URL:
Abubakar N, Ilyasu Y, Samaila MO, Bappa AU, Akpobi KC, Samdi MT. Epithelioid hemangioma mimicking multinodular goiter: A case report and the review of the literature. Niger J Surg Res [serial online] 2016 [cited 2018 Jul 21];17:14-6. Available from: http://www.njsrjournal.org/text.asp?2016/17/1/14/182475 |
| Introduction | |  |
Sharon Weiss and Franz Enzinger first described epithelioid hemangioma (EH) in 1969 as a benign vascular tumor that usually occurs in the skin and subcutis. It has previously been called by many names.[1],[2] Goiter is a common endemic disease in our setting thus neck masses are likely to be misdiagnosed based on clinical history and examination alone. The diagnosis of EH is also frequently being used for vascular lesions of the bone.[3],[4],[5] We present a 55-year-old female with anterolateral neck mass simulating goiter.
| Case Report | | |
A 55-year-old female presented to the surgical outpatient clinic of our teaching hospital with 15 years history of neck mass. The mass was not associated with pain, dysphagia or syncope attacks. There was also no history of proptosis or weight loss. Her past medical history was not contributory. Clinical examination showed a well-preserved afebrile, anicteric female with a huge multinodular anterior neck mass extending to the left sternocleidomastoid muscle. The mass measured 15 cm × 14 cm × 5 cm and was soft to firm in consistency. There were no other palpable masses detected. Based on her clinical history and examination, a diagnosis of multinodular goiter with malignant degeneration was made. She was counseled and prepared for surgery. Her full blood count and chemistry were within the normal limit for age and sex. Thyroid function tests showed thyroid-stimulating hormone - 2.8 µIu/ml, T3-1.1 ng/ml and T4-70 ng/ml, all within the reference range. Intraoperatively, a deep-seated solid-cystic mass encasing vascular channels was seen. The mass measured 16 cm × 14 cm × 4.5 cm and contained 30 ml of hemorrhagic fluid. The thyroid gland was intact and uninvolved. The excised mass was submitted to the pathology laboratory for histological analysis.
We received in 10% formol saline an irregularly shaped grey-tan firm mass weighing 284 g and measuring 14 cm × 13 cm × 4.5 cm. It's cut surfaces showed solid and multilocular cystic areas, with the largest cyst measuring 6 cm in its widest diameter. The tissue was processed in paraffin and stained with hematoxylin and eosin. Microscopy revealed proliferating small, capillary-sized vessels lined by plump endothelial cells with eosinophilic cytoplasm and an inflammatory rich stroma composed predominantly of lymphocytes forming follicles and eosinophils [Figure 1] and [Figure 2]. Some of the vessels were cystically dilated whereas others were congested. Other areas show skeletal muscle bundles and lobules of mature adipocytes. There was no thyroid tissue seen. Immunohistochemical staining for CD34 showed strong reactivity [Figure 3] and [Figure 4] and a diagnosis of EH was made.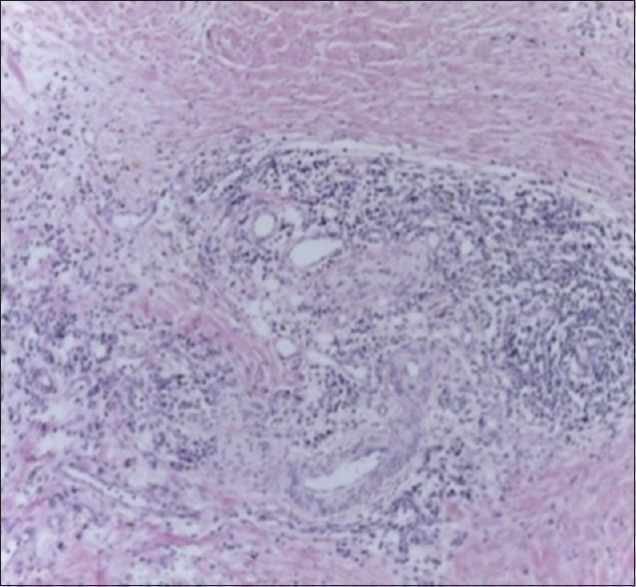 | Figure 1: Numerous vascular channels lined by epithelioid endothelial cells (H and E, ×40)
Click here to view |
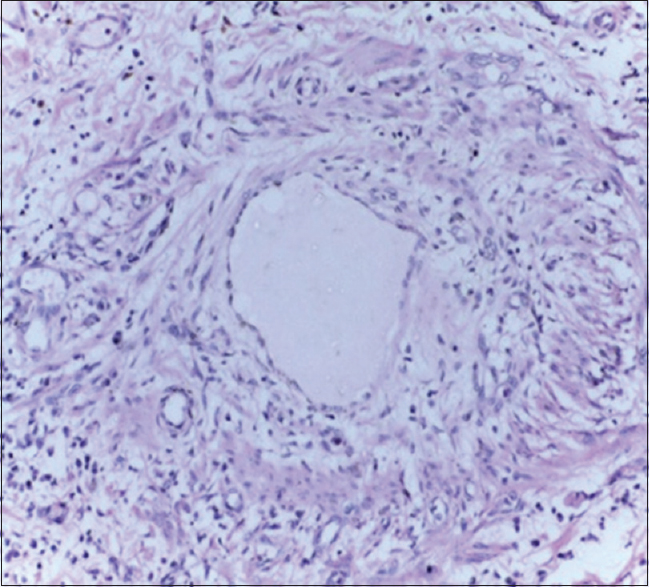 | Figure 2: Proliferating vascular channels lined by epithelioid endothelial cells (H and E, ×100)
Click here to view |
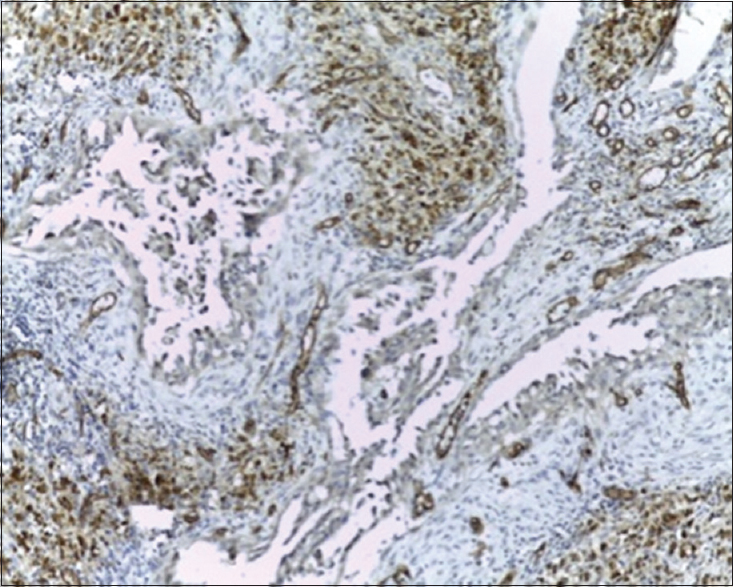 | Figure 3: Positive immunohistochemical staining for CD34 antibody (IHC, ×40)
Click here to view |
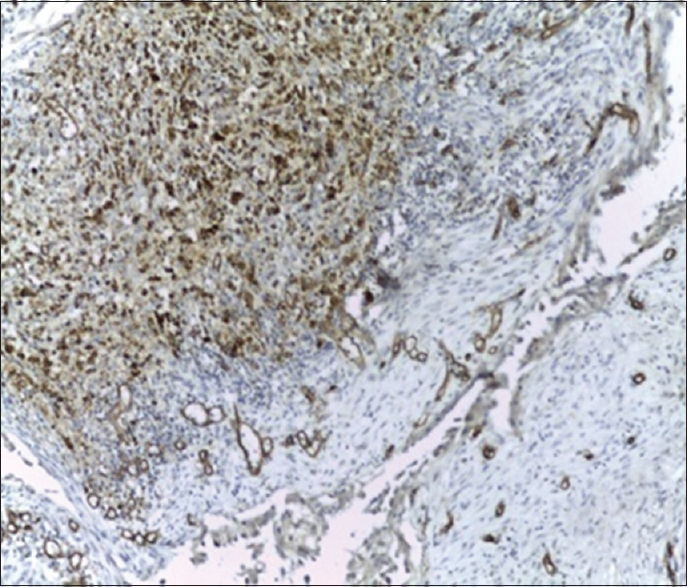 | Figure 4: Positive immunohistochemical stain for CD 34 antibody (IHC, ×100)
Click here to view |
| Discussion | | |
EH, also called by various names,[3],[6],[7] is a benign vascular lesion that runs an indolent clinical course. It is occasionally associated with the multifocal presentation and a rare metastatic potential to locoregional lymph nodes.[4],[8] EH has a female predilection due to estrogen and progesterone, with some of the cases occurring during or shortly after pregnancy.[9] The peak age of affectation is in the third to fifth decades.[3],[10] The most frequently affected sites are the forehead, preauricular area and scalp often in the distribution of the superficial temporal artery. Other sites include the neck and the distal extremities.[3],[7] Its location in the anterior neck in the index case led to the erroneous clinical diagnosis of multinodular goiter which is a very common disease in our setting. The supportive clinical finding for goiter was the gender of the patient, location, and size of the mass Although the thyroid function tests were not deranged and should have raised a flag of misdiagnosis.
The neck is not an uncommon site of occurrence of EH, but the long duration in the index case, the multilobulated presentation with cystic degeneration and the deep-seated location is a source of misdiagnosis. The majority of patients present with a nodular mass of less than a year duration with localization in the subcutis. The dermal presentation is infrequent while deep-seated lesions as in the index case are rare and affects large vessels.[3],[5],[7],[10],[11] The most frequent preoperative clinical impressions include epidermal cyst and angioma.[3] A differential of multinodular goiter is not out of place in endemic areas, especially with the size of the mass.
There remains considerable controversy as to whether EH is a reactive lesion or a true neoplasm.[3] EH is characterized histologically by a prominent proliferation of small, capillary-sized vessels lined by plump, epithelioid endothelial cells. The vessels have an immature appearance and lack a well-defined lumen though well formed with single cell layering of the endothelium and an entire myopericytic layer. The endothelial cells have amphophilic or eosinophilic cytoplasm that may be vacuolated. The lesion is usually well demarcated from the surrounding soft tissue and commonly centered around a large muscular artery.[6],[7],[8],[10] The stroma shows an inflammatory milieu rich in eosinophils and lymphocytes with prominent lymphoid follicle formation.[3],[8],[12] EH must be distinguished from other vascular lesions such as epithelioid hemangioendothelioma or an epithelioid angiosarcoma and other nonneoplastic processes such as bacillary angiomatosis and Kimura's disease. The epithelioid endothelial cells of EH are immunoreactive for CD31, CD34 and factor VIIIrAg. Keratin expression may also be detected. Immunostaining for alpha-smooth muscle actin or muscle specific actin is helpful in demonstrating an entire myopericytic layer around the immature vessels. Complete local excision is the optimal treatment for EH although local recurrence is seen in one-third of patients.[3],[4],[10] Goiter on the other hand present with dominant clinical features caused by the mass effects of the enlarged gland such as airway obstruction, dysphagia, and compression of large vessels in the neck and upper thorax (superior vena cava syndrome) and even in euthyroid forms features are confirmed histologically.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | |
| 2. | Kurihara Y, Inoue H, Kiryu H, Furue M. Epithelioid hemangioma (angiolymphoid hyperplasia with eosinophilia) in zosteriform distribution. Indian J Dermatol 2012;57:401-3.  [ PUBMED]  |
| 3. | Fletcher CD, Unni KK, Mertens F, editors. Pathology and Genetics of Tumours of Soft Tissue and Bone; World Health Organiszation Classification of Tumours. Lyon: IARC Press; 2002. |
| 4. | Nielsen GP, Srivastava A, Kattapuram S, Deshpande V, O'Connell JX, Mangham CD, et al. Epithelioid hemangioma of bone revisited: A study of 50 cases. Am J Surg Pathol 2009;33:270-7. |
| 5. | O'Connell JX, Kattapuram SV, Mankin HJ, Bhan AK, Rosenberg AE. Epithelioid hemangioma of bone. A tumor often mistaken for low-grade angiosarcoma or malignant hemangioendothelioma. Am J Surg Pathol 1993;17:610-7. |
| 6. | Al-Daraji WI, Prescott RJ, Abdellaoui A, Khan MM, Kulkarni K, Youssef MM, et al. Cutaneous epithelioid angiomatous nodule: Different views or interpretations in the analysis of ten new cases. Dermatol Online J 2009;15:2. |
| 7. | Olsen TG, Helwig EB. Angiolymphoid hyperplasia with eosinophilia. A clinicopathologic study of 116 patients. J Am Acad Dermatol 1985;12(5 Pt 1):781-96. |
| 8. | Errani C, Zhang L, Panicek DM, Healey JH, Antonescu CR. Epithelioid hemangioma of bone and soft tissue: A reappraisal of a controversial entity. Clin Orthop Relat Res 2012;470:1498-506. |
| 9. | Lamovec J, Bracko M. Epithelioid hemangioma of small tubular bones: A report of three cases, two of them associated with pregnancy. Mod Pathol 1996;9:821-7. |
| 10. | Sharon WW, John RG. Enzinger and Weiss's Soft Tissue Tumors. 4 th ed. Atlanta: Trazandeh Medical Pub.; 2001. |
| 11. | Tyring S, Guest P, Lee P, Little W, Jaffe K, Pritchett R. Epithelioid hemangioendothelioma of the skin and femur. J Am Acad Dermatol 1989;20(2 Pt 2):362-6. |
| 12. | Ismail M, Damato S, Freeman A, Nigam R. Epithelioid hemangioma of the penis: Case report and review of literature. J Med Case Rep 2011;5:260. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|









 Search Pubmed for
Search Pubmed for