|
 
 |
| CASE REPORT |
|
| Year : 2016 | Volume
: 17
| Issue : 1 | Page : 23-26 |
|
A rare case of strangulated obturator hernia presenting as subacute intestinal obstruction
Suvendu Maji, Makhan Lal Saha, Tanveer Adil, Soumen Das
Department of General Surgery, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India
| Date of Web Publication | 16-May-2016 |
Correspondence Address:
Suvendu Maji
Department of General Surgery, Institute of Postgraduate Medical Education and Research, Room No. 230, 244 AJC Bose Road, PG Hostel, Kolkata - 700 020, West Bengal
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/1595-1103.182477

An obturator hernia is a rare condition but is associated with the highest mortality of all abdominal wall hernias. They are notorious for their diagnostic difficulty and present a challenge to the surgeon. Preoperative diagnosis is often a rarity. They commonly present in elderly emaciated women, typically associated with chronic diseases. The most common symptom is strangulation combined with mechanical intestinal obstruction. Early surgical intervention is often delayed due to the absence of clinical and radiological clues. The following case report highlights these difficulties and reviews current literature on the management of such cases. Keywords: Intestinal obstruction, obturator hernia, strangulation
How to cite this article:
Maji S, Saha ML, Adil T, Das S. A rare case of strangulated obturator hernia presenting as subacute intestinal obstruction. Niger J Surg Res 2016;17:23-6 |
How to cite this URL:
Maji S, Saha ML, Adil T, Das S. A rare case of strangulated obturator hernia presenting as subacute intestinal obstruction. Niger J Surg Res [serial online] 2016 [cited 2018 Jul 21];17:23-6. Available from: http://www.njsrjournal.org/text.asp?2016/17/1/23/182477 |
| Introduction | |  |
An obturator hernia is a type of pelvic hernia, in which a bowel segment protrudes through the obturator foramen adjacent to the obturator vessels and nerve. It occurs more frequently in patients with ascites, chronic constipation, and chronic obstructive pulmonary disease and in thin elderly multiparous women.[1] The risk of strangulation in such hernias is high. Signs and symptoms are often vague and nonspecific. Because of the diagnostic difficulty, they often present late and diagnosis is mostly made intraoperatively. Since they occur in elderly ladies with comorbidities, the morbidity and mortality rates are also high.
Herein, we describe a case of an elderly lady who presented to us with features of subacute intestinal obstruction secondary to a strangulated obturator hernia.
| Case Report | | |
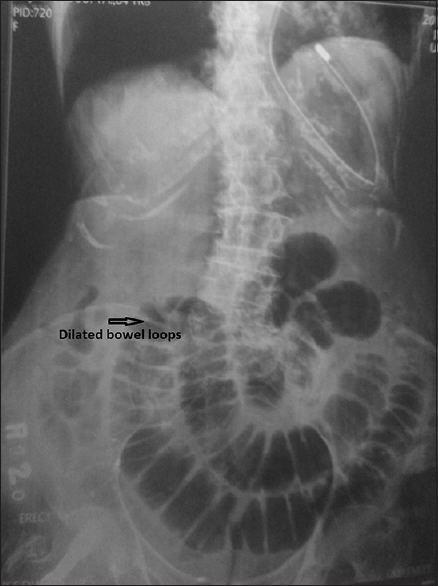
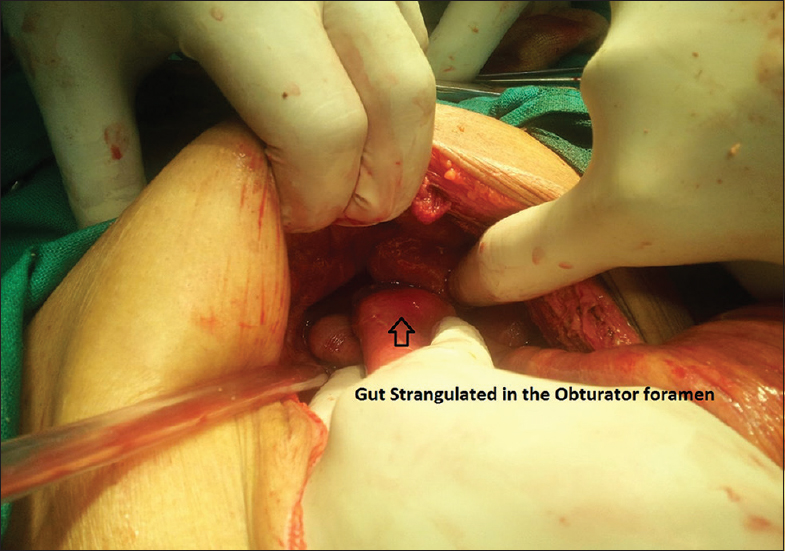
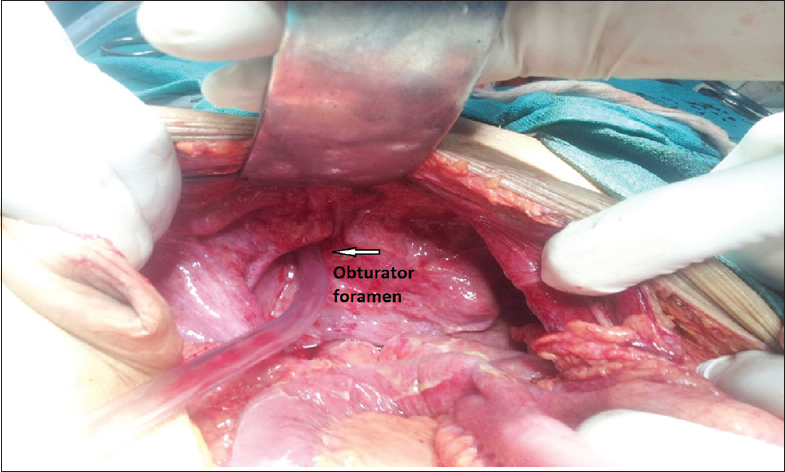
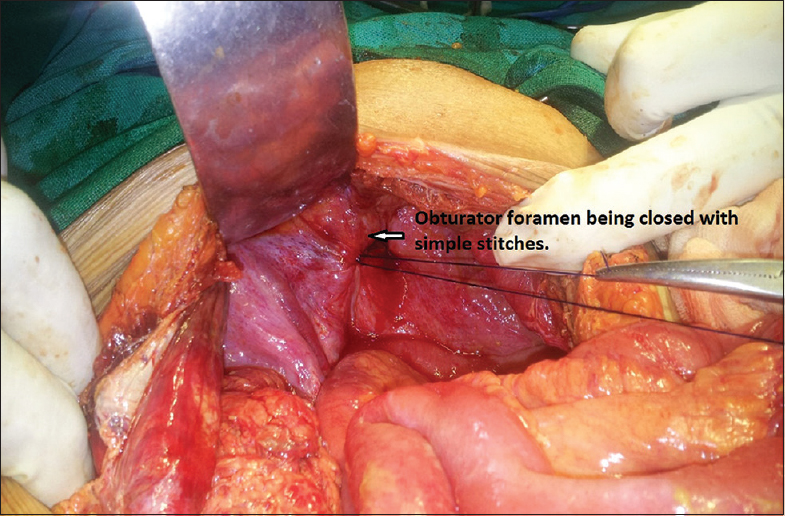
A 77-year-old thin and frail lady presented to us with 7 days history of intermittent pain of the abdomen and few episodes of nausea and vomiting. The patient was apparently well a week before when she experienced an acute episode of pain in her left groin, for which she was admitted in a private hospital. There she was given conservative treatment, and routine investigations were done. However, her condition did not improve; rather she started experiencing pain all over her abdomen. Same evening, she was admitted into Seth Sukhlal Karnani Memorial Hospital on an emergency basis. She did not complain of constipation, obstipation, abdominal swelling, or discomfort. Her past history revealed she had two such similar episodes of diffuse pain of the abdomen 6 months back, which resolved with self-medication of nonsteroidal anti-inflammatory drugs. She denied any antecedent history of abdominal operation. On admission, she was alert and conscious but was restless. She had no signs of dehydration, and her vitals were stable. Physical examination revealed generalized abdominal tenderness and abdominal distension with muscle rigidity. No abdominal lump was palpable, and examination of her groins did not reveal any swelling. There was no visible bowel peristalsis. On auscultation, bowel sounds were absent. Per rectal and per vaginal examination was unremarkable. Her body weight was 39 kg. Her hemoglobin was 13 g/dl, and white blood count was 9000/cumm. Her serum electrolytes were within normal limits. Ultrasound of the whole abdomen demonstrated features of sub acute intestinal obstruction with mild ascites. The plain x-ray of the abdomen showed multiple dilated loops of small bowel located in the central part of the abdomen [Figure 1]. She was taken up for exploratory laparotomy. Under general anesthesia, the abdomen was opened through a midline incision. Thorough exploration was done. Abdomen was found to be filled with flakes of fibrin and features of generalized peritonitis were present. Peritoneal lavage with normal saline was done. A portion of the small gut was found to have entered the left obturator canal [Figure 2] and [Figure 3]. The gut was gently pulled out. However, a portion of it was found to be strangulated. Resection of the gangrenous gut was done, and an ileostomy was performed. The obturator foramen was closed with simple prolene sutures [Figure 4]. Abdomen was closed in layers. Ileostomy closure was done 6 weeks later. The patient was fine at the end of 7 months follow-up and had no recurrences.
| Discussion | | |
An obturator hernia was initially described by Arnaud de Ronsil in 1724 and was first successfully repaired in 1851 by Henry Obre. It is an uncommon problem that occurs predominantly in elderly, debilitated women. Incidence rates vary widely throughout the world but range from 0.073% to 1.0% of all hernias and 0.2–1.6% of all cases of mechanical obstruction.[1] It occurs through the obturator canal, which is approximately 2–3 cm long and 1 cm wide. Obturator hernias are much more common in elderly female and postpregnancy patients owing to the greater width of the pelvis, larger obturator canal, and increased laxity of the pelvic tissues.[2] The condition has been nicknamed the “little old ladies hernia” as it affects this group due to atrophy and loss of the preperitoneal fat around the obturator vessels in the canal predisposing hernia formation. The hernia proceeds through the obturator foramen situated bilaterally in the anterolateral pelvic wall, inferior to the acetabulum. The obturator nerves and vessels pass through this tunnel, protected by extraperitoneal connective tissue and fat. Emaciation and advanced age cause the loss of this tissue as evidenced by most patients being in their seventh and eighth decades.
The symptoms are vague and are usually in the form of nausea and vomiting or other signs of bowel obstruction such as abdominal pain and a lack of bowel movement. The literature has shown that up to 80% of patients with obturator hernias usually have symptoms of bowel obstruction, which is often partial due to a high proportion exhibiting Richter's herniation of the bowel into the obturator canal.[3] This tends to give rise to a clinical picture of intermittent bowel obstruction symptoms, which is an important factor to identify in the clinical history if an accurate diagnosis is to be made. Compression of the obturator nerve by the hernial sac produces the pathognomonic Howship-Romberg sign shown to be present in 15–50% of obturator hernia cases.[3] This referred pain is relieved by flexion of the thigh and exacerbated by abduction, extension, and medial rotation. The loss of adductor reflex is due to compression of the obturator nerve and has been termed as Hannington-Kiff sign. These signs are often absent, as in our case or overlooked because of low index of suspicion. Abdominal radiography is most often nonspecific showing features of bowel obstruction as seen in our case.
Recent literature has shown that early diagnosis of an obturator hernia can be made with computed tomography (CT) scan of the abdomen and pelvis.[4],[5] However, an emphasis is also placed on the dangers of over-reliance on such imaging. Our case demonstrates that radiological and operative findings may not always correlate and that only intraoperatively can a truly accurate diagnosis be made. Despite this, the consensus from current published evidence is that CT of the pelvis and upper thigh is the most useful imaging tool when an obturator hernia is suspected clinically. CT imaging of bowel herniating through the obturator foramen and lying between the pectineus and obturator muscles is shown to be the best diagnostic clue.[6] The management of an obturator hernia is surgical. However, few case reports of nonoperative management have also been described in the literature. Various surgical approaches have been described in the literature in the acute management of an obturator hernia. Abdominal, inguinal, retropubic, obturator, and laparoscopic approaches have all been described. The majority of published evidence favors the abdominal approach, utilizing a low midline incision. This method allows the surgeon to establish the diagnosis, avoid any obturator vessels, give better exposure of the obturator ring, and facilitate bowel resection, if necessary.[7] Simple closure of the hernial defect, with interrupted sutures or placement of a synthetic mesh, are the preferred methods of herniorrhaphy as they are associated with the lowest complication.
The literature on laparoscopic repair of obturator hernias is quite sparse, probably due to a combination of the rarity of these cases and the relatively recent emergence of laparoscopic hernia surgery. Both transabdominal and extra-peritoneal laparoscopic approaches have been described in the literature.[7],[8],[9] Laparoscopic repair has been shown to produce less postoperative pain, fewer pulmonary complications, and shorter hospital stays in such cases. Given these results, and the fact that obturator hernias classically tend to occur in patients that have limited physiological reserve, an argument could be made for a shift in practice from open repairs toward laparoscopic repairs.[10]
| Conclusion | | |
It should be kept in mind that an obturator hernia is a rare but significant cause of intestinal obstruction, especially in emaciated elderly women. Detailed history taking and physical examination provide diagnostic clue for suspected obturator hernia. CT scan is valuable to establish preoperative diagnosis. Early diagnosis and prompt surgical treatment are essential to reduce the morbidity and mortality.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Bjork AKJ, Cahill DR. Obturator hernia. Surg Gynecol Obstet 1988;167:217-22.  |
| 2. | De Clerq L, Coenegrachts K, Feryn T, Van Couter A, Vandevoorde P, Verstraete K. An elderly woman with obstructed obturator hernia: A less common variety of external abdominal hernia. Journal Belge de Radiologie – Belgisch Tijdschrift voor Radiologi 2010;93:302-4. |
| 3. | Mantoo SK, Mak K, Tan TJ. Obturator hernia: Diagnosis and treatment in the modern era. Singapore Medical Journal 2009;50:866. |
| 4. | Yokoyama Y, Yamaguchi A, Isogai M, Hori A, Kaneoka Y. Thirty-six cases of obturator hernia: Does computerised tomography contribute to postoperative outcome? World Journal of Surgery 1999;23:2144-7. |
| 5. | Dundamadappa SK, Tsou IY, Goh JS. Clinics in diagnostic imaging. Singapore Medical Journal 2006;47:88-94. |
| 6. | Jamadar D, Jacobson J, Morag Y, Girish G, Ebrahim F, Gest T. Sonography of inguinal region hernias. American Journalism Review 2006;187:185-90. |
| 7. | Moreno-Egea A, La Calle MC, Torralba-Martinez JA. Obturator hernia as a cause of chronic pain after inguinal hernioplasty: Elective management using tomography and ambulatory total extraperitoneally laparoscopy. Surgical Laparoscopy Endoscopy & Percutaneous Techniques 2006;16:54-7. |
| 8. | Wu JM, Lin HF, Chen KH, Tseng LM, Huang SH. Laparoscopic pre-peritoneal mesh repair of incarcerated obturator hernia and contralateral direct inguinal hernia. Journal of Laparoendoscopic & Advanced Surgical Techniques A. 2006;16:616-9. |
| 9. | Hunt L, Morrison C, Lengyel J, Sagar P. Laparoscopic management of an obstructed obturator hernia: Should laparoscopic assessment be the default option? Hernia 2009;13:313. |
| 10. | Hodgins N, Cieplucha K, Conneally P, Ghareeb E. Obturator hernia: A case report and review of the literature. International Journal of Surgery Case Reports 2013;4:889-92. doi:10.1016/j.ijscr.2013.07.012. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|









 Search Pubmed for
Search Pubmed for