|
 
 |
| CASE REPORT |
|
| Year : 2016 | Volume
: 17
| Issue : 1 | Page : 20-22 |
|
Peyronie's disease and erectile dysfunction: A case report and review of literature
Olajide Olusegun Abiola1, Ibukun Olalekan Oyinloye2, Segun Oladele Adeniyi1
1 Department of Surgery, Urology Unit, Bowen University Teaching Hospital, Ogbomoso, Oyo, Nigeria
2 Department of Radiology, University of Ilorin Teaching Hospital, Ilorin, Kwara, Nigeria
| Date of Web Publication | 16-May-2016 |
Correspondence Address:
Olajide Olusegun Abiola
Department of Surgery, Urology Unit, Bowen University Teaching Hospital, P. O. Box 15, Ogbomoso, Oyo
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/1595-1103.182483

Peyronie's disease (PD) is characterized by fibrous plaque deposit in the tunica albuginea of corpus cavernosum, which may be associated with penile pain, deformities, and erectile dysfunction (ED). Its prevalence in Nigeria is not known, but limited numbers of cases were reported in literature. However, improvement in the management of ED has led to an increase in the presentation of patients with ED to physicians; in which during evaluation of such patients, PD has been occasionally diagnosed. This case report highlights the clinical findings and management of a Nigerian adult male who presented with erectile failure with clinical findings of PD and literature review of PD associated with ED. Keywords: Erectile dysfunction, Nigerian men, Peyronie's disease
How to cite this article:
Abiola OO, Oyinloye IO, Adeniyi SO. Peyronie's disease and erectile dysfunction: A case report and review of literature. Niger J Surg Res 2016;17:20-2 |
How to cite this URL:
Abiola OO, Oyinloye IO, Adeniyi SO. Peyronie's disease and erectile dysfunction: A case report and review of literature. Niger J Surg Res [serial online] 2016 [cited 2018 Jul 21];17:20-2. Available from: http://www.njsrjournal.org/text.asp?2016/17/1/20/182483 |
| Background | |  |
Peyronie's disease (PD) is characterized by deposit of fibrous plaque in the tunica albuginea of corpus cavernosum, which can be accompanied by pain on penile erection, penile deformity or penile lump, difficulty in penetrative sexual intercourse, erectile dysfunction (ED), and can be of psychological distress to patients and their partners.[1],[2]
Global prevalence is unknown, but a prevalence rate of 3.2% was reported in a population survey in Europe [3] and a lesser prevalence of 0.6% was reported in Japanese men.[4] However, its prevalence in Nigerian men is unknown with only few cases documented in literature.[5],[6]
Recently, more cases are being diagnosed globally; this was attributed to the advent of potent drugs treatment of ED as many incidental cases were diagnosed during evaluation of men with ED.[3],[7]
We report a case of PD and ED in a Nigerian man with a literature review of the diagnosis and management of the disease.
| Case Report | | |
A 56-year-old Nigerian man presented with complaint of failure to maintain penile erection of 2 months duration. This was associated with penile pain and subsequent flail distal penile shaft during an attempt at sexual intercourse.
There was no prior trauma to the penile shaft and no previous history of penile or perineal surgery. He had no urethral instrumentation or catheterization in the past and his urinary stream was normal.
He was a known diabetic diagnosed 2 years earlier with good blood sugar control and also being managed for gout over the last 10 years.
He was not a known hypertensive patient and had no history of intermittent claudication in the extremities.
An assessment of ED with International Index of Erectile Function (IIEF)-5 score of 14 (moderate ED) was made.
He was obese (body mass index of 32.4 kg/m 2) with circumcised male external genitalia; a hard lump was felt at the left dorsal aspect of the penile shaft.
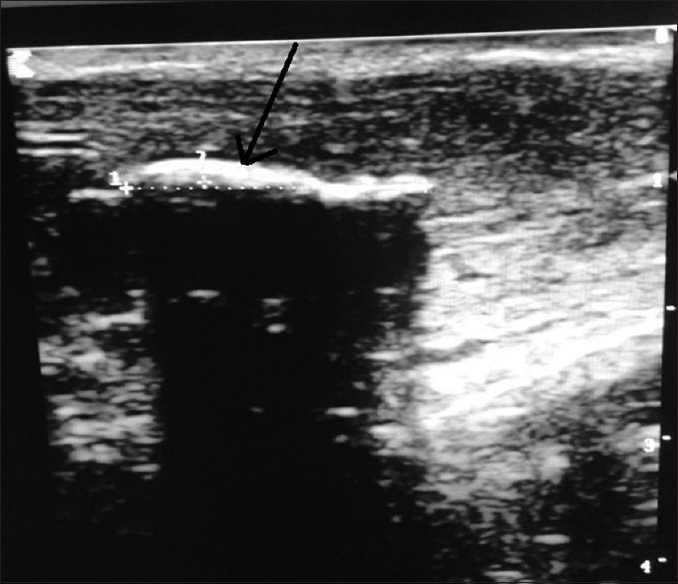
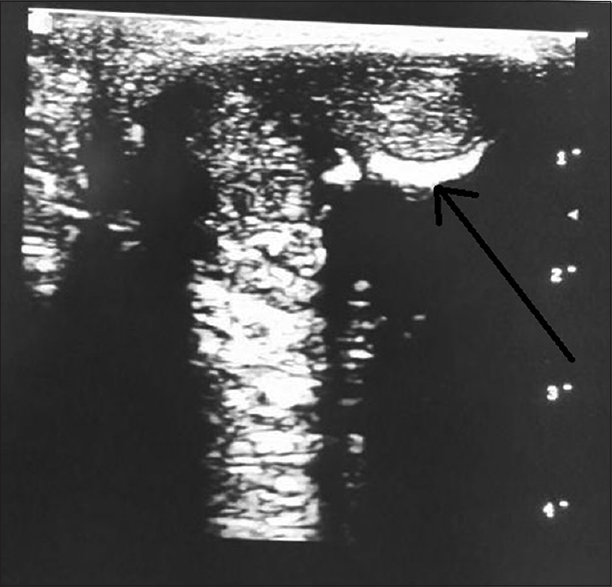
Penile ultrasound scan revealed hyperechoic region at the left dorsal aspect of corpus cavernosum casting an acoustic shadow [Figure 1]; on transverse scan – thickened hyperechoic region at the dorsal margin of left corpus cavernosum with reduced girth [Figure 2].
A diagnosis of ED with PD was made. He had medical therapy with Tamoxifen and Vitamin E at a dose of 20 mg b.i.d and 200 mg daily, respectively.
On re - evaluation after 3 months of medical therapy, he reported reduced penile pain on erection with improved erectile function (IIEF -5 score was 22 - mild ED). He is still being followed up on treatment.
| Discussion | | |
In Nigeria, only a few cases of PD have been reported in literature.[5],[6] These limited cases of PD in Nigerian men may be due to similar factors earlier reported as reasons for low prevalence of the disease in other countries rather than rarity of the disease. These include failure to diagnose the disease in men with ED, patients' reluctance to report to physician because of the embarrassment of penile deformity, and also limited number of patients report their ED to physicians.[8]
PD is usually found in men in their fifties.[9] The etiology is still unknown, but several authors have attributed different causative factors which include penile trauma associated with delaminating injuries to tunica albuginea and wound healing disorders, genetics, auto immune disorders, connective tissue disorders (Dupuytren's contracture), and vascular disorders.[9],[10],[11]
Risk factors that have been reported are diabetes mellitus and gout as in the case of this report. Hypertension, Dupuytren's contracture, dyslipidemia, smoking, penile trauma during sexual intercourse, urethral catheterization/manipulation, and pelvic surgeries are other proposed risk factors.[9],[12]
The natural history of the disease is often progressive in nature. The disease is classified into two phases; an active phase that is characterized by increasing plaque size, penile curvature, and pain- usually last 12–18 months from onset of the disease. The chronic phase is characterized by absence of penile pain, unchanging penile curvature, and plaque size.[10]
Clinical presentation of PD includes penile lump, painful penile erection, penile deformity, flail penis on erection, and ED.[13]
In the index patient, the presentation was ED with flail penis and pain on erection with an incidental finding of penile lump on examination. Such finding of penile lump suggestive of PD is not unusual in patients with ED. A study in Turkey revealed an incidental PD in 16% of men being evaluated for ED.[7]
Predisposing factors to ED in patients with PD include penile deformity and pain, which may affect sexual function; performance anxiety due to penile deformity; and embarrassment in the presence of his partner.[14]
Diagnosis of PD is essentially clinical. However, further investigation may be required to demonstrate the fibrous plaque at the tunica albuginea and assess penile vasculature using Doppler ultrasound, especially when there is associated ED.[15],[16]
Penile ultrasound demonstrates the plaque as focal thickening of tunica albuginea - A hyperechoic region, which cast an acoustic shadow when calcified as seen in our patient.[15]
Magnetic resonance imaging gives a better penile image resolution, especially with plaque at the penile base;[17] however, its major drawback is the poor demonstration of calcified plaque compared to ultrasonography.[15]
Management of patient with PD associated with ED should be individualized. Medical therapy with follow-up could be considered in the early phase of the disease.[10],[11] These medical therapies include oral pharmacotherapy such as Vitamin E and Tamoxifen, which were used in the treatment of the index patient. Other oral medications for the treatment of PD include colchicine, acetyl-L carnitine, pentoxifylline, and potassium para-aminobenzoate. Topical therapy with verapamil and intralesional injection therapy with verapamil, nicardipine, steroids, clostridial collagenase, or interferon alpha 2β as a form of medical therapy have also been used.[11]
Forms of nonoperative therapy reported include the use of extracorporeal shock wave therapy, transdermal electromotive administration of drugs: Iontophoresis and penile traction systems.[11]
Surgical treatment is usually indicated at the chronic phase in patients with severe PD preventing intromission, failed medical therapy, and for cosmetic reasons.[10] Such surgical procedures include plaque excision with plication (Nesbit), plaque excision with grafting, and penile prosthesis implantation.
Surgical therapy of PD with associated ED should be cautiously selected to avoid worsening of the ED. Studies have shown that Nesbit procedure tends to be associated with the least postoperative ED although associated with penile shortening, while men with penile shortening but with good erectile function will benefit more with plaque excision and grafting. Penile prosthesis implantation is best reserved for men with associated severe ED.[18]
| Conclusion | | |
With advancements in the management of ED, more patients are likely to present to physicians for the treatment of their ED. A high index of suspicion on the possible coexistence of PD in patients with ED will help in the diagnosis and improve the outcome of treatment for the ED.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Jalkut M, Gonzalez-Cadavid N, Rajfer J. Peyronie's disease: A review. Rev Urol 2003;5:142-8.  |
| 2. | Rosen R, Catania J, Lue T, Althof S, Henne J, Hellstrom W, et al. Impact of Peyronie's disease on sexual and psychosocial functioning: Qualitative findings in patients and controls. J Sex Med 2008;5:1977-84. |
| 3. | Sommer F, Schwarzer U, Wassmer G, Bloch W, Braun M, Klotz T, et al. Epidemiology of Peyronie's disease. Int J Impot Res 2002;14:379-83. |
| 4. | Shiraishi K, Shimabukuro T, Matsuyama H. The prevalence of Peyronie's disease in Japan: A study in men undergoing maintenance hemodialysis and routine health checks. J Sex Med 2012;9:2716-23. |
| 5. | Takure AO, Atalabi OM. Management and outcome of Peyronie's disease in Nigeria – Initial experience. Niger J Surg 2011;17:87-9.  |
| 6. | Aisuodionoe-Shadrach OI. The burden of specialist urologic care in Abuja, federal capital city, Nigeria: A single surgeons 4-year case load. West Afr J Med 2012;31:92-6. |
| 7. | Kadioglu A, Oktar T, Kandirali E, Kendirci M, Sanli O, Ozsoy C. Incidentally diagnosed Peyronie's disease in men presenting with erectile dysfunction. Int J Impot Res 2004;16:540-3. |
| 8. | Levine LA, Latchamsetty KC. Treatment of erectile dysfunction in patients with Peyronie's disease using sildenafil citrate. Int J Impot Res 2002;14:478-82. |
| 9. | Kadioglu A, Tefekli A, Erol B, Oktar T, Tunc M, Tellaloglu S. A retrospective review of 307 men with Peyronie's disease. J Urol 2002;168:1075-9. |
| 10. | Smith JF, Walsh TJ, Lue TF. Peyronie's disease: A critical appraisal of current diagnosis and treatment. Int J Impot Res 2008;20:445-59. |
| 11. | Kuehhas FE, Weibl P, Georgi T, Djakovic N, Herwig R. Peyronie's disease: Nonsurgical therapy options. Rev Urol 2011;13:139-46. |
| 12. | Carrieri MP, Serraino D, Palmiotto F, Nucci G, Sasso F. A case-control study on risk factors for Peyronie's disease. J Clin Epidemiol 1998;51:511-5. |
| 13. | Pryor JP, Ralph DJ. Clinical presentations of Peyronie's disease. Int J Impot Res 2002;14:414-7. |
| 14. | Pryor JP. Peyronie's disease and impotence. Acta Urol Belg 1988;56:317-21. |
| 15. | Kalokairinou K, Konstantinidis C, Domazou M, Kalogeropoulos T, Kosmidis P, Gekas A. US imaging in Peyronie's disease. J Clin Imaging Sci 2012;2:63. [ PUBMED] |
| 16. | Pawlowska E, Bianek-Bodzak A. Imaging modalities and clinical assesment in men affected with Peyronie's disease. Pol J Radiol 2011;76:33-7. |
| 17. | Vossough A, Pretorius ES, Siegelman ES, Ramchandani P, Banner MP. Magnetic resonance imaging of the penis. Abdom Imaging 2002;27:640-59. |
| 18. | Pryor J, Akkus E, Alter G, Jordan G, Lebret T, Levine L, et al. Peyronie's disease. J Sex Med 2004;1:110-5. |
[Figure 1], [Figure 2]
|









 Search Pubmed for
Search Pubmed for