|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2016 | Volume
: 17
| Issue : 1 | Page : 5-9 |
|
Bacterial flora in precataract surgery patients in a Northern Nigerian hospital
AF Mahmud-Ajeigbe1, KK Oladigbolu1, FJ Giwa2, ER Abah1, AL Rafindadi1, AT Olayinka2, VA Pam1
1 Department of Ophthalmology, Ahmadu Bello University Teaching Hospital, Shika-Zaria, Nigeria
2 Department of Microbiology, Ahmadu Bello University Teaching Hospital, Shika-Zaria, Nigeria
| Date of Web Publication | 16-May-2016 |
Correspondence Address:
K K Oladigbolu
Department of Ophthalmology, Ahmadu Bello University Teaching Hospital, Shika-Zaria
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/1595-1103.182481

Background: Cataract surgery is the most commonly performed surgery in most ophthalmic units. Endophthalmitis is still a dreaded complication and knowledge of the normal bacterial flora on the ocular surface and adnexae is paramount in the management of these cases.
Aims and Objectives: To investigate the most frequently found ocular bacteria flora in patients scheduled for routine cataract surgery at the Ahmadu Bello University Teaching Hospital Shika Zaria, Northern Nigeria and to determine their antimicrobial susceptibility pattern.
Materials and Methods: This was a cross-sectional descriptive study carried out between December 2010 and February 2012 in subjects scheduled to undergo routine cataract surgery. The lower conjunctival fornix was swabbed with a sterile swab. The samples were inoculated onto enriched and selective culture media. Antimicrobial susceptibility testing was done using the modified Kirby Bauer standardized disc-diffusion method. Data were entered and analyzed using SPSS version 20.0.
Results: One hundred and fifty-seven eyes of 157 patients were sampled. The patients were between the ages of 16–96 years with a mean age of 58.8 ± 14.5 years. Positive bacterial culture was found in 35% (n = 55) of the patients. The predominant bacteria cultured was Staphylococcus epidermidis 49.1%. There was resistance to tetracycline (32.7%) and gentamycin (1.8%). All the isolates were sensitive to tobramycin and ciprofloxacin. A statistically significant relationship was found between age and culture status (P = 0.008).
Conclusion: Coagulase negative Staphylococcus (S. epidermidis) was the most common commensal found in the conjunctival sacs of patients undergoing cataract surgery, and most of the isolates were susceptible to commonly used antibiotics. Keywords: Antibiotic sensitivity, cataract, conjunctival flora
How to cite this article:
Mahmud-Ajeigbe A F, Oladigbolu K K, Giwa F J, Abah E R, Rafindadi A L, Olayinka A T, Pam V A. Bacterial flora in precataract surgery patients in a Northern Nigerian hospital. Niger J Surg Res 2016;17:5-9 |
How to cite this URL:
Mahmud-Ajeigbe A F, Oladigbolu K K, Giwa F J, Abah E R, Rafindadi A L, Olayinka A T, Pam V A. Bacterial flora in precataract surgery patients in a Northern Nigerian hospital. Niger J Surg Res [serial online] 2016 [cited 2018 Jul 21];17:5-9. Available from: http://www.njsrjournal.org/text.asp?2016/17/1/5/182481 |
| Introduction | |  |
It is estimated that about 48% of global blindness is due to cataract. In Nigeria cataract is said to account for 43% of blindness and 45.3% of severe visual impairment.[1] It is not surprising that cataract surgery is the most common surgery performed in most eye units in Nigeria and around the globe.[2] Every type of surgery has its attendant complications, and one of the most devastating complications of cataract surgery is postoperative endophthalmitis. Although rare, this condition with an incidence of between 0.05% and 0.265%[3],[4],[5] can cause profound visual loss in as much as 80% of cases.[6]
Potential sources of causative organisms in cases of postoperative endophthalmitis include peri-ocular flora of patients, contaminated surgical intraocular instruments, and contaminated environment.[7],[8],[9] Bacteria in the conjunctival sac have been found to play a role in its pathogenesis.[10],[11],[12],[13],[14] Studies have reported the presence of bacterial colonies in the conjunctival sac of 55–100% of normal patients preoperatively.[15],[16]
Conjunctival culture is not routinely done in patients undergoing cataract surgery in the study area. Preventive measures routinely carried out against postoperative endophthalmitis include the instillation of 5% povidone-iodine drops into the conjunctival fornix of all patients, ensuring strict maintenance of aseptic technique during surgery and the use of intra and postoperative antibiotics. Studies have demonstrated the effectiveness of 5% povidone-iodine aqueous solution for the eradication of pathogenic bacteria such as Streptococcus pneumoniae, Staphylococcus aureus, Actinomyces pyogenes, Actinomyces meiyeri and Actinomyces odontolyticus in the conjunctival surface. There is also a significant reduction in the quantities of Staphylococcus epidermidis and Micrococcus luteus which are the commonly isolated bacteria flora in the conjunctiva.[17]
The normal conjunctival flora develops following birth and the pattern continues to change throughout life.[18],[19] The pattern of conjunctival flora varies with the environment, age, sex, season, body resistance, and general hygienic conditions.[20] Rational use of prophylactic antibiotics is dependent on the knowledge of the resident conjunctival flora and its sensitivity pattern in that environment. This serves as an important tool in the management of patients undergoing cataract surgery or other intraocular surgery.
This study aims to investigate the most frequently found ocular bacteria flora in patients scheduled for routine cataract surgery at the Ahmadu Bello University Teaching Hospital Shika Zaria, Northern Nigeria and to determine their antimicrobial susceptibility pattern.
| Materials and Methods | | |
This was a cross-sectional descriptive study carried out between December 2010 and February 2012. The subjects were 16 years and above who were scheduled to undergo routine cataract surgery. Excluded were patients with any form of active ocular infection or inflammation, history or presence of blepharitis or conjunctivitis. Also excluded were patients who had previous use of topical eye drops or ointment and systemic antibiotics within the last 3 months. All patients gave full written informed consent, ethical clearance was obtained from the Hospital Ethical Committee and the study was carried out according to the Helsinki declaration.
Only one eye of each of the subjects was sampled (i.e., the eye undergoing surgery). The lower conjunctival fornix was swabbed with a sterile swab. Employing a continuous stroke from the nasal to the temporal side, the swab was rolled to the other side and another stroke was done from the temporal to nasal side. One of the investigators took all the samples with the aid of sterile gloves, a face mask and a cap. No anesthetic or disinfecting agents were used on the eyes before sample collection. The samples were taken directly to the microbiology laboratory and inoculated within 15–30 min of collection.
The samples were directly inoculated onto enriched (Blood and Chocolate (Oxoid Ltd., England) and selective (MacConkey (Oxoid Ltd., England) culture media and were incubated in carbon dioxide enriched and aerobic atmospheres respectively at 35°C for 24–48 h. A smear was also made from the swab and a primary Gram-stain done. Cultures positive for bacterial growth were secondarily Gram-stained and further identified and characterized using colonial morphology, conventional biochemical tests, and analytical profile index (API ® Staph. Kit [Biomerieux]). All bacterial isolates were tested for susceptibility to antimicrobials using the modified Kirby-Bauer standardized disc-diffusion method.
Antibiotic susceptibility testing
The antibiotic susceptibility testing was carried out using the modified Kirby-Bauer disc-diffusion method as specified by the Clinical and Laboratory Standards Institute (CLSI, 2011). Antimicrobial agents used in testing were chloramphenicol 30 µg, gentamycin 10 µg, erythromycin 5 µg, tetracycline 30 µg, penicillin G 10 µg, tobramycin 10 µg, and ciprofloxacin 5 µg. All plates were incubated at 35°C for 18–24 h. The diameters of zones of inhibition were measured using a ruler to the nearest millimeter and compared and interpreted using the CLSI Interpretative chart (2011) as S (susceptible), I (intermediate) or R (resistant). S. aureus ATCC 25923 strain was used as quality control. Data was entered and analyzed using SPSS version 20.0 (SPSS Inc., Chicago, IL, USA). Where necessary, the Fisher's exact and Chi-square test were used to determine any significant difference with a P < 0.05 considered statistically significant.
| Results | | |
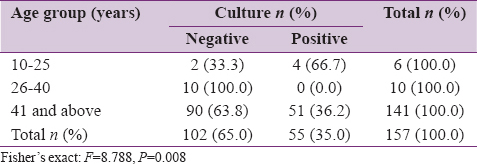
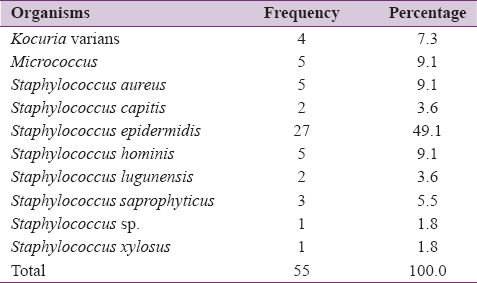
We sampled 157 eyes of 157 patients. The patients were between the ages of 16–96 years with a mean age of 58.8 ± 14.5 years [Table 1] and a male to female ratio of 2.3:1 [Table 2]. Positive bacterial culture was found in 35% (n = 55) of the patients [Table 1] and [Table 2], 65.4% (n = 36) of these were patients above 60 years [Table 1]. All the bacteria cultured were Gram-positive. Majority (74.5%, n = 41) of the organisms cultured were coagulase-negative Staphylococcus (CoNS) [Table 3].
The predominant bacteria isolated was S. epidermidis which made up 65.8% (n = 27) of the CoNS and 49.1% (n = 27) of the total organisms cultured. This was followed by S. aureus, Staphylococcus hominis and Micrococcus sp. each making up 9.1% (n = 5) of the bacteria cultured [Table 3]. A statistically significant relationship was found between culture status and age (P = 0.008), as well as sex (P = 0.01).
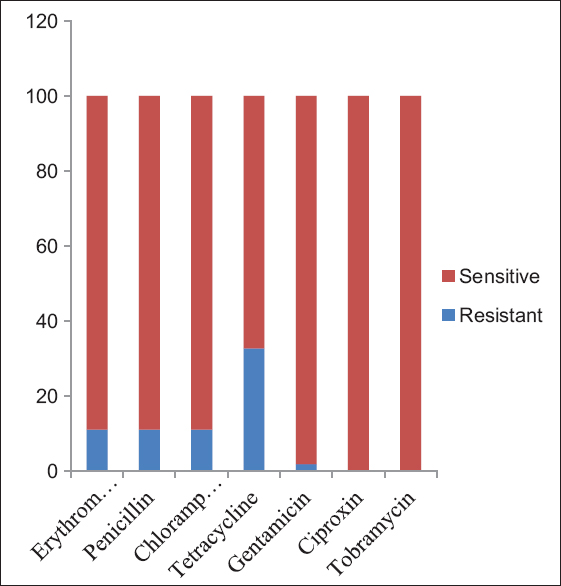
Antimicrobial susceptibility testing was done using erythromycin 5 µg, penicillin g 10 µg, chloramphenicol 30 µg, tetracycline 30 µg, gentamycin 10 µg, ciprofloxacin 5 µg and tobramycin 10 µg discs. Out of the bacterial isolates cultured, 32.7% (n = 18) showed resistance to tetracycline. Resistance each to erythromycin, chloramphenicol and penicillin was found in 11% (n = 6) of the isolates and gentamycin resistance was found in 1.8% (n = 1) of the isolates cultured. All the isolates were sensitive to tobramycin and ciprofloxacin [Figure 1]. There were no multidrug-resistant organisms.
| Discussion | | |
In this study, 35% (n = 55) of the subjects had a positive culture. Studies carried out here in Nigeria, and other parts of the world show a variation in positive cultures of preoperative conjunctival isolates ranging from 30% to 90%.[6], 8, [21],[22],[23]
CoNS made up 74.5% (n = 41) of the isolates which was similar to de Kaspar et al.[21] and Mistlberger et al.[22] who had CoNS as 76% and 75% of their isolates in their study. This is probably because the studies were done at base hospitals following similar procedures to our study. The study in Ife, Nigeria [23] CoNS made up 50% of the isolates which is lower, while Chung et al.[24] in Korea had a higher value of 85%. Though in a study of the lid (closely related to the conjunctiva) Bekibele et al.[13] found CoNS made up 70% of the bacterial isolates. This finding is most likely because the eyelids serve as filters for particles and debris attempting to enter the eyes, untrapped materials which eventually get into the conjunctival fornix will be similar to those filtered by the lids.
In the current study, 65.4% (n = 36) of patients that had positive culture were above 60 years. This is similar to Suto et al. in Japan [6] who found that 79% of those with a positive culture were 60 years and over and also Omotoye in Ife [23] who found that 64% of patients with a positive culture were ≥50 years. The reduced personal hygiene of visually challenged elderly persons, as well as reduced immunity, could be responsible for this finding as immune function decreases with normal aging.[25] The high isolation rate in patients ≥60 years means they are more susceptible to post-operative infection and should, therefore, have more aggressive preoperative prophylaxis.
In our study, we did not culture any Gram-negative organisms while most similar studies done show low rates of isolation of Gram-negative. Suto et al., de Kaspar et al. and Omotoye had 6.7%, 5.9%, and 29.5%, respectively.[6],[21],[23] With regards to antibiotic sensitivity, we found that all the bacterial isolates were sensitive to ciprofloxacin and tobramycin. This was in contrast to studies from other parts of the world were there seems to be a growing resistance by organisms to the older fluoroquinolones. Suto et al.[6] found a 14% resistance to ciprofloxacin and de Kaspar et al.[21] found as much as 81% resistance to levofloxacin. Suto et al.[6] also found a 17.9% resistance to tobramycin whereas we found none. This can be explained by the relatively higher cost of these antibiotics in the study area making the likelihood of abuse less and by extension lower resistance by the organisms. Resistance to Gentamycin was found in 1.8% (n = 1) of the organisms which compares with a study by Omotoye [23] who found 82.6% of their isolates sensitive to gentamycin, 11% (n = 6) of organisms were resistant to erythromycin which is comparable to what Omotoye [23] found in 29% of their isolates. de Kaspar et al.[21] however found resistance in 50% of their isolates.
Chloramphenicol which is commonly used had an 11% (n = 6) resistance from the isolates in contrast to Omotoye in Ife who found a 61.3% resistance to chloramphenicol.[23] Tetracycline had resistance from 32.7% (n = 18) of isolates which is about half the proportion of Omotoye who found 71% of isolates resistant to this drug.[23] CoNS are the most prevalent bacteria in the conjunctival sac with S. epidermidis being the most common. Commonly used antibiotics such as chloramphenicol, gentamycin, ciprofloxacin, and tobramycin are still generally effective against these resident flora.
| Conclusion | | |
CoNS are the most prevalent bacteria in the conjunctival sac with S. epidermidis being the most common. The high isolation rate in patients ≥ 60 years means they are more susceptible to postoperative infection and should, therefore, have more aggressive preoperative prophylaxis. Commonly used antibiotics such as chloramphenicol, gentamycin, ciprofloxacin, and Tobramycin are still generally effective against these resident flora.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Rabiu MM, Kyari F, Ezelum C, Elhassan E, Sanda S, Murthy GV, et al. Review of the publications of the Nigeria national blindness survey: Methodology, prevalence, causes of blindness and visual impairment and outcome of cataract surgery. Ann Afr Med 2012;11:125-30.  [ PUBMED]  |
| 2. | Adio AO. Surgical uptake in an ophthalmically underserved state in Nigeria: A preliminary Report. J Surg Surg Sci2008;1:24-8. |
| 3. | Speaker MG, Milch FA, Shah MK, Eisner W, Kreiswirth BN. Role of external bacterial flora in the pathogenesis of acute postoperative endophthalmitis. Ophthalmology 1991;98:639-49. |
| 4. | Hori Y, Nakazawa T, Maeda N, Sakamoto M, Yokokura S, Kubota A, et al. Susceptibility comparisons of normal preoperative conjunctival bacteria to fluoroquinolones. J Cataract Refract Surg 2009;35:475-9. |
| 5. | Lalitha P, Rajagopalan J, Prakash K, Ramasamy K, Prajna NV, Srinivasan M. Postcataract endophthalmitis in South India incidence and outcome. Ophthalmology 2005;112:1884-9. |
| 6. | Suto C, Morinaga M, Yagi T, Tsuji C, Toshida H. Conjunctival sac bacterial flora isolated prior to cataract surgery. Infect Drug Resist 2012;5:37-41. |
| 7. | 7. Walker CB, Claoué CM. Incidence of conjunctival colonization by bacteria capable of causing postoperative endophthalmitis. J R Soc Med 1986;79:520-1. |
| 8. | Liesegang TJ. Use of antimicrobials to prevent postoperative infection in patients with cataracts. Curr Opin Ophthalmol 2001;12:68-74. |
| 9. | Miño de Kaspar H, Grasbon T, Kampik A. Automated surgical equipment requires routine disinfection of vacuum control manifold to prevent postoperative endophthalmitis. Ophthalmology 2000;107:685-90. |
| 10. | Kazmierczak AK, Szewczyk EM. Bacteria forming a resident flora of the skin as a potential source of opportunistic infections. Pol J Microbiol 2004;53:249-55. |
| 11. | Gawronska M, Kaluzny J, Mikucka A, Gospodarek E. Bacterial flora of conjunctival sac in patients with cataract. Methods of disinfection and evaluation of their efficiency. Klin Oczna 2005;107:408-13. |
| 12. | Dohmen PM. Influence of skin flora and preventive measures on surgical site infection during cardiac surgery. Surg Infect (Larchmt) 2006;7 Suppl 1:S13-7. |
| 13. | Bekibele CO, Kehinde AO, Ajayi BG. Upper lid skin bacterial count of surgical eye patients in Ibadan, Nigeria. Afr J Med Med Sci 2008;37:273-7. |
| 14. | Heaven CJ, Mann PJ, Boase DL. Endophthalmitis following extracapsular cataract surgery: A review of 32 cases. Br J Ophthalmol 1992;76:419-23. |
| 15. | Boes DA, Lindquist TD, Fritsche TR, Kalina RE. Effects of povidone-iodine chemical preparation and saline irrigation on the perilimbal flora. Ophthalmology 1992;99:1569-74. |
| 16. | Singer TR, Isenberg SJ, Apt L. Conjunctival anaerobic and aerobic bacterial flora in paediatric versus adult subjects. Br J Ophthalmol 1988;72:448-51. |
| 17. | Vanzzini Zago V, Villar-Kuri J, Flores-Alvarado V, Marino Castro A, Pérez-Balbuena AL. Conjunctival flora before and after application of 5% povidone-iodine solution. Open Access Textbook: Conjunctivitis – A Complex and Multifaceted Disorder, Part 3. Ch. 9. Rijeka, Croatia: InTech Open Access Publisher; 2011. p. 135-44. |
| 18. | Gündüz A, Gündüz A, Cumurcu T, Seyrek A. Conjunctival flora in Behçet patients. Can J Ophthalmol 2008;43:476-9. |
| 19. | Thiel HJ, Schumacher U. Normal flora of the human conjunctiva: Examination of 135 persons of various ages. Klin Monbl Augenheilkd 1994;205:348-57. |
| 20. | Kanellopoulos AJ, Dreyer EB. Postoperative infection following current cataract extraction surgery. Int Ophthalmol Clin 1996;36:97-107. |
| 21. | de Kaspar HM, Kreidl KO, Singh K, Ta CN. Comparison of preoperative conjunctival bacterial flora in patients undergoing glaucoma or cataract surgery. J Glaucoma 2004;13:507-9. |
| 22. | Mistlberger A, Ruckhofer J, Raithel E, Müller M, Alzner E, Egger SF, et al. Anterior chamber contamination during cataract surgery with intraocular lens implantation. J Cataract Refract Surg 1997;23:1064-9. |
| 23. | Omotoye OJ. Conjunctival Bacterial Colonization of Cataract Patients in OAUTHC Ile-Ife, Fellowship Dissertation for the National Postgraduate Medical College Nigeria; 2010. |
| 24. | Chung JL, Seo KY, Yong DE, Mah FS, Kim TI, Kim EK, et al. Antibiotic susceptibility of conjunctival bacterial isolates from refractive surgery patients. Ophthalmology 2009;116:1067-74. |
| 25. | Cannizzo ES, Clement CC, Morozova K, Valdor R, Kaushik S, Almeida LN, et al. Age-related oxidative stress compromises endosomal proteostasis. Cell Rep 2012;2:136-49. |
[Figure 1]
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for