|
 
 |
| CASE REPORT |
|
| Year : 2016 | Volume
: 17
| Issue : 2 | Page : 58-60 |
|
Utero-cutaneous fistula following cesarean section
Matthew Chum Taingson, Joel A Adze, Stephen B Bature, Amina Mohammed Durosinlorun, Mohammed Caleb, Abubakar Amina
Department of Obstetrics and Gynaecology, Faculty of Medicine, Barau Dikko Teaching Hospital, Kaduna State University, Kaduna, Nigeria
| Date of Web Publication | 16-Nov-2016 |
Correspondence Address:
Matthew Chum Taingson
Department of Obstetrics and Gynaecology, Faculty of Medicine, Barau Dikko Teaching Hospital, Kaduna State University, Kaduna
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/1595-1103.194212

Utero-cutaneous fistula is an extremely rare entity, and only a few case reports have been published. Most Utero-cutaneous fistulas are secondary to postpartum or postoperative complications. A 23-year-old woman, para 1+0, not alive, noticed bleeding through her abdominal incision scar, following a cesarean section for retained second twin 5 years before presentation. A fistulous tract was demonstrated at examination under anesthesia with a probe, between the uterus and wound. The patient had laparotomy with excision of the fistulous tract and uterine repair; she did well postoperatively. Although our patient had a successful surgical treatment, prevention of utero-cutaneous fistula by meticulous technique during the primary surgical procedure and measures to prevent postoperative sepsis would have spared this patient the distress, cost, and risk of a second operation. Keywords: Cesarean section, uterine repair, utero cutaneous fistula
How to cite this article:
Taingson MC, Adze JA, Bature SB, Durosinlorun AM, Caleb M, Amina A. Utero-cutaneous fistula following cesarean section. Niger J Surg Res 2016;17:58-60 |
How to cite this URL:
Taingson MC, Adze JA, Bature SB, Durosinlorun AM, Caleb M, Amina A. Utero-cutaneous fistula following cesarean section. Niger J Surg Res [serial online] 2016 [cited 2018 Jul 21];17:58-60. Available from: http://www.njsrjournal.org/text.asp?2016/17/2/58/194212 |
| Introduction | |  |
Utero-cutaneous fistula is a rare occurrence. It is an abnormal communication between two epithelial surfaces, the uterus and skin.[1] Most utero-cutaneous fistulas develop secondary to postpartum or postoperative complications. Other possible causes of this rare occurrence are intrauterine devices and endometriosis.[2]
| Case Report | | |
Mrs. S. S. a 23-year-old para 1+0 housewife with no formal education, presented at the Barau Dikko Teaching Hospital Kaduna State, Nigeria, on 23rd of October 2015, with a 5-year history of bloody discharge during her menstrual period from the mid-line incision scar of a cesarean section, she had had for a retained twin. Surgery was complicated by postoperative wound sepsis. She went into preterm labor at 30 weeks and delivered the leading twin male stillbirth spontaneously. However, the second twin was retained and had to be delivered by an emergency cesarean section 20 h later. The second twin, also a male, died 25 h after birth.
She attained menarche at the age of 13 years and menstruated for 5 days in a 28-day regular cycle. She had no prior problems with irregular or heavy menses.
On examination, she was a young woman afebrile (temp 37°C), anicteric, and not pale. There was no pedal edema. The respiratory rate was 22 cycles/min. Her pulse rate was 90 beats per min, regular and good volume, and blood pressure 110/70 mmHg.
Abdominal examination revealed a low midline subumbilical scar about 8 cm in length with puckering in its midpoint. A fistulous opening about 1–2 mm in diameter was at the midpoint of the scar [Figure 1]a and [Figure 1]b. Pelvic examination revealed no abnormal findings.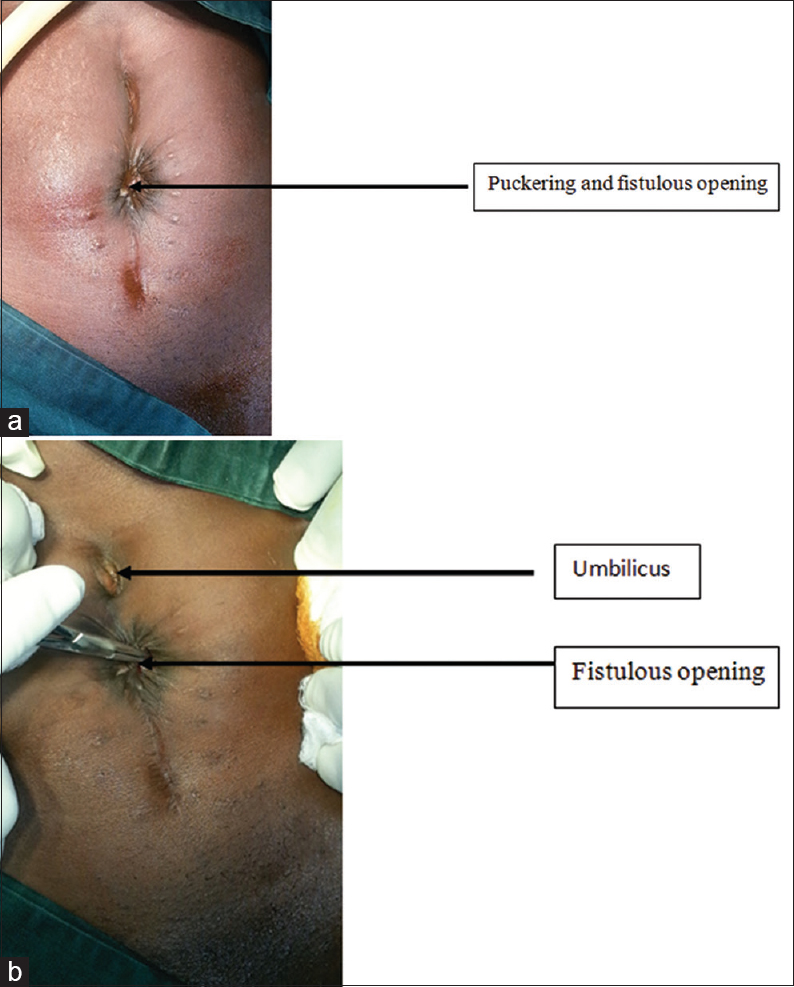 | Figure 1: (a) The fistulous opening in the abdominal incision scar, (b) the fistulous opening in the abdominal incision scar
Click here to view |
On investigation, her hematocrit was 31%, and her serum electrolytes, urea, and creatinine levels were essentially normal. Abdominopelvic scan showed an empty uterus 3 cm in length, with endometrial plate visualized and adnexa normal. Hysterosalpingography (HSG) showed an elongated cervix with uterine cavity located around the second and third lumbar vertebra, fallopian tubes difficult to assess, but free contrast spillage bilaterally noted.
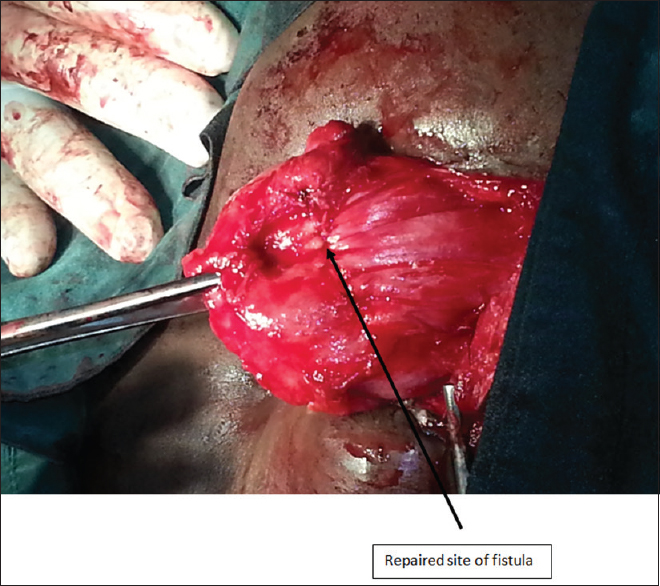
She had laparotomy under general anesthesia. Intraoperative, the bladder, a loop of small bowel, and omentum were found to be adherent to previous cesarean scar on the mid-anterior uterine wall. There was a 3-cm sinus tract extending from previous cesarean scar on the uterus to peritoneum, rectus sheath onto the skin [Figure 2]a. Adhesiolysis with the freeing of the uterus, omentum, bladder, bowel followed by fistulectomy was performed, a bluish tinge opening of the fistulous tract on the uterus was seen [Figure 2]b. The uterus was then repaired in layers [Figure 3]. She had an uneventful recovery and was discharged on postoperative day 5. She was seen at the gynecology outpatient clinic 6 weeks later, and her clinical condition was found satisfactory. Histopathology of the fistulous tract showed fibromuscular tissue, and the tract lined by granulation tissue with nonspecific inflammation.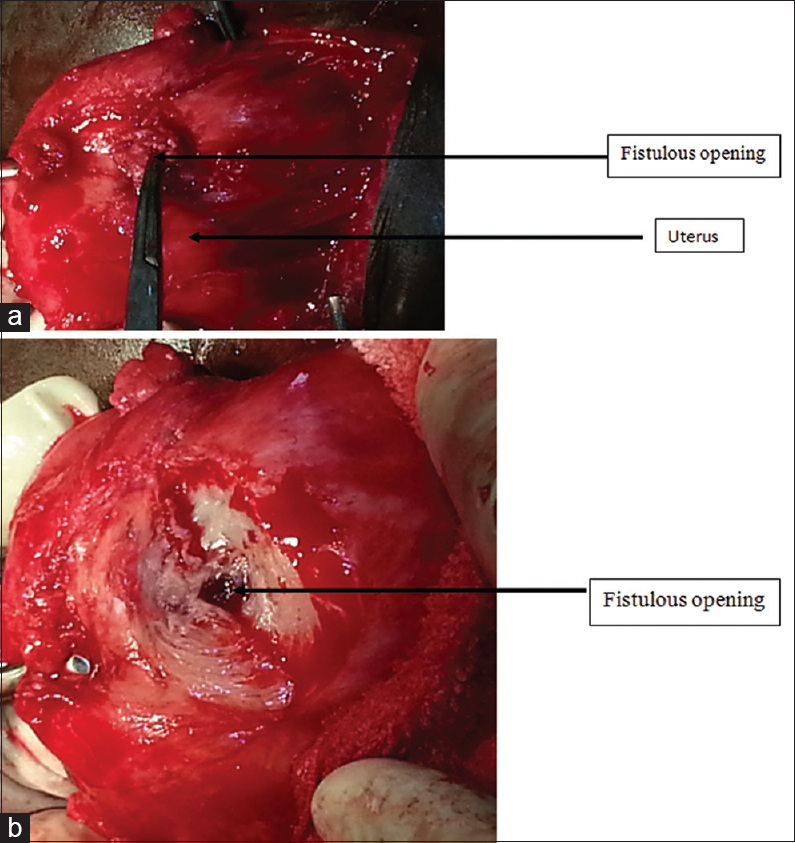 | Figure 2: (a) Distal end of fistulous tract on the uterus, (b) a bluish tinge on the uterine muscle around fistulous tract
Click here to view |
| Discussion | | |
Utero-cutaneous fistula usually results from postpartum or postoperative complications. Most fistulae originate from trauma, or some other type of inflammatory processes that disrupt the continuity of tissues involved. The decrease in the incidence of utero-abdominal fistula may reasonably be attributed to marked decrease in the frequency of classical cesarean section in modern obstetrics.[3],[4] Utero-cutaneous fistula following lower segment cesarean section has been reported.[5] Gupta et al. reported utero-cutaneous fistula which developed following septic abortion induced by laminaria tent insertion in the cervix.[1] Review of literature also revealed possible risk factors: history of multiple abdominal surgeries, use of drains, incomplete closure of uterine wound following cesarean, intra-abdominal sepsis in previous scar, and secondary abdominal pregnancy.
In our case, the patient had a sinus at the midportion of midline scar. She might have developed this complication due to placement of the uterine scar on the upper uterine segment as the surgery was done at 30 weeks of gestation, and the lower uterine segment is not well formed at that gestational age. This site of incision is prone to adhesion formation. Ascending infection from home delivery of the first twin and delivery interval of about 20 h would have contributed to postoperative wound sepsis.
Demonstration of the fistulous tract can be done with a dye injected transcervically, fistulogram, HSG, contrast-enhanced computed tomography (CT) scan, and magnetic resonance imaging (MRI). Our patient had a HSG done; however, the fistulous tract was not demonstrated. This shortcoming in the use of HSG and fistulogram has been reported.[6],[7] Contrast CT scan and MRI could have depicted the tract; they were not available in our hospital at that time.
Once a fistula is diagnosed, the basic principle in treatment is obliteration of opening of fistulous tract [8] as done in our case by excision and uterine repair.
Complete closure of the uterine wound in two layers using absorbable suture, avoid inclusion of decidua during closure, and proper tissue handling to prevent ischemia would go a long way in preventing this catastrophe.
| Conclusion | | |
The case highlights this rare complication of cesarean section. It also emphasizes the need for competence at cesarean section and measures to prevent postoperative sepsis.
Acknowledgment
The authors would like to express gratitude to Prof. Lydia Airede for her critical reading and comments on the case report.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Gupta SK, Shukla VK, Varma DN, Roy SK. Uterocutaneous fistula. Postgrad Med J 1993;69:822-3.  |
| 2. | Dragoumis K, Mikos T, Zafrakas M, Assimakopoulos E, Stamatopoulos P, Bontis J. Endometriotic uterocutaneous fistula after cesarean section. A case report. Gynecol Obstet Invest 2004;57:90-2. |
| 3. | Dessouky DA, Bolan J. Uteroabdominal sinus following cesarean section. Am J Obstet Gynecol 1980;137:147-8. |
| 4. | Jain V, Jain SS. Post cesarean uterocutaneous fistula – A rare clinical entity. J Obstet Gynecol India 2003;53:97. |
| 5. | Yadav P, Gupta S, Singh P, Tripathi S. Successful medical management of uterocutaneous fistula. Int J Gynaecol Obstet 2014;124:263-4. |
| 6. | Abasiattai AM, Ibanga GJ, Akpan A, Ume KU. Post caesarean section uterocutaneous fistula: A case report. J Womens Health Issues 2014;3:5. |
| 7. | Lim PS, Shafiee MN, Ahmad S, Hashim Omar M. Utero-cutaneous fistula after caesarean section secondary to red degeneration of intramural fibroid. Sex Reprod Healthc 2012;3:95-6. |
| 8. | Yadav R, Reddi Rani P, Jayalakshmi D. Uterocutaneous fistula. J Obstet Gynecol India 2006;56:81-2. |
[Figure 1], [Figure 2], [Figure 3]
|









 Search Pubmed for
Search Pubmed for