|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2016 | Volume
: 17
| Issue : 2 | Page : 53-57 |
|
Pattern of traumatic spinal cord injury in Makurdi, Nigeria
Williams Terhemen Yongu, Cornelius Itodo Elachi, Daniel Demesugh Mue, Joseph Aluetse Kortor
Department of Surgery, College of Health Sciences, Benue State University Teaching Hospital, Makurdi, Benue State, Nigeria
| Date of Web Publication | 16-Nov-2016 |
Correspondence Address:
Williams Terhemen Yongu
College of Health Sciences, Benue State University Teaching Hospital, Benue State
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/1595-1103.194219

Objectives: To study the pattern of presentation and outcome of conservative treatment of traumatic spinal cord injury (TSCI) in our institution.
Setting: Benue State University Teaching Hospital, Makurdi, Benue State.
Materials and Methods: A 3-year retrospective review (June 2012 to May 2015) of TSCI was done. Demographic data, cause, associated injuries, time interval to presentation, level of injury, American Spinal Injury Association (ASIA) classification at presentation and at 6 weeks were obtained from case notes. The patients were all managed conservatively and had bed rest on air or water mattress.
Results: There were 45 patients mean age 33.26 ± 1.55 (range 8–77 years) with TSCI comprising 37 males and 8 females giving a male: female ratio of 4.6:1. Students were mostly affected (n = 11, 24%) while motor vehicular accident was the cause of injury (n = 18, 40%). Cervical spine was the most injured (n = 24 53.3%). Majority had the ASIA Class A (n = 22 48.9%) at presentation. Thirteen (48.1%) of them improved, two were referred, six remained the same, eight deteriorated, and 16 were discharged against medical advice. Period of hospitalization was 1–65 days.
Conclusion: TSCI affects mainly young males involved in motor vehicular accident. Conservative treatment can be used in resource-constrained centers. Keywords: Conservative care, Nigeria, spinal cord injury
How to cite this article:
Yongu WT, Elachi CI, Mue DD, Kortor JA. Pattern of traumatic spinal cord injury in Makurdi, Nigeria. Niger J Surg Res 2016;17:53-7 |
| Introduction | |  |
Traumatic spinal cord injury (TSCI) is a major cause of morbidity and mortality worldwide. Trauma to the vertebral column may affect the spinal cord resulting in a change, either temporarily or permanently, in the cord's normal motor, sensory, or autonomic function. Common causes of TSCI are motor vehicular crashes (MVCs), gunshot, falls, sports injuries, occupational injuries, assault, and diving into shallow waters. In Nigeria, TSCI is also associated with a significant morbidity and mortality.[1],[2],[3],[4],[5],[6],[7],[8] The socioeconomic realities, inadequate immediate attendant care, and the near-absent rehabilitation of people with spinal cord injury (SCI) may be responsible for poor outcome of the treatment in the developing countries.[9] As a result of the weak rehabilitation facilities, patients develop preventable complications while on admission thereby prolonging hospital stay and constituting a financial burden on them. Studies have identified many risk factors [10],[11],[12] for morbidity and mortality in SCI, but many of these risk factors have not been studied in the developing world.
SCI patients often require extended treatment in specialized Spinal Unit or an Intensive Care Unit. The rehabilitation process following a SCI typically begins in the acute care setting. A combined team of orthopedic surgeons, plastic surgeons, physical therapists, occupational therapists, nurses, social workers, psychologists, and other health-care professionals typically work together to decide on goals with the patient and develop a plan of discharge that is appropriate for the patient's condition.
SCI mainly affects young people, mostly males, causing a significant morbidity with huge human and economic losses. This is because most victims are left with permanent disability and may require specialist care for the rest of their lives.[13],[14] It is estimated that there are 40,000 patients in the UK with SCI, giving a prevalence of 1 in 1500 (0.7%) patients.[15] There is paucity of comparative epidemiological data on the incidence and prevalence of SCI in Nigeria, due to lack of case registers at local, state, and federal level.
We conducted this study to provide information on TSCI in Makurdi, North Central Nigeria, and outcome of conservative care.
| Materials and Methods | | |
A 3-year retrospective (June 2012 to May 2015) review was done at Benue State University Teaching Hospital. It is one of the three tertiary institutions in the state and has four orthopedic surgeons who manage musculoskeletal trauma as well as orthopedic cases. The information on age, sex, occupation, cause, associated injuries, time interval to presentation, level of injury, neurological deficit, American Spinal Injury Association (ASIA) class at presentation and at 6 weeks, radiological findings, complications at presentation and at 6 weeks, as well as outcome, was obtained from case notes in the medical records department. Inclusion criteria were patients who sustained TSCI and presented within 6 weeks to our center. The patients who had older injuries (>6 weeks) were excluded from the study. All the patients were managed conservatively with cervical collar or skull traction, thoracolumbar brace or jacket, and lumbar brace when indicated. Drugs such as nonsteroidal anti-inflammatory drugs, paracetamol, antibiotics, and oxygen were given when indicated. All the patients had bed rest on air or water mattresses throughout their period of admission.
The three outcome measures at discharge were categorized as “improved” if they increased by at least one class on their ASIA classification within 6 weeks. “Same” are those whose ASIA class did not change throughout the period of treatment. “Deteriorated” are in-hospital patients whose conditions worsened within the first 6 weeks. Discharged against medical advice are those who requested for discontinuation of their treatment earlier than six weeks and eventually left the hospital even after the consequences of their action has been explained to them. They were not considered for analysis of outcome. Six weeks were used as cutoff mark because at this point in the treatment of spinal cord injured patient, the vertebrae which are cancellous bone are expected to have healed. Neurological improvement in those that would improve also shows appreciable, measurable progress. The patients can be discharged at this stage with neck collars or Minerva jacket or lumbar corset and/or wheelchair depending on level and severity of injury.
Data were analyzed using the Statistical Package for Social Sciences 17.0 (SPSS Inc., Chicago, IL, USA); continuous variables are presented as means ± standard deviation, whereas categorical variables are presented as frequencies.
| Results | | |
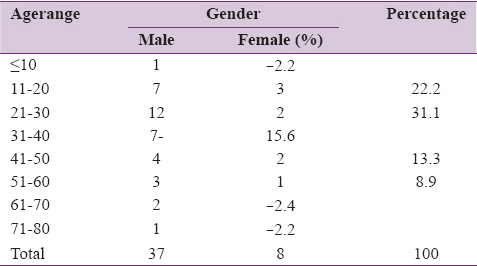
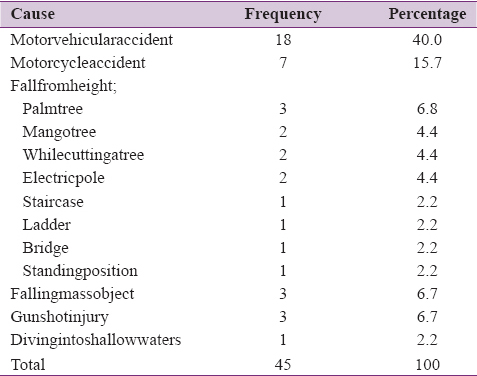
There were 45 patients mean age 33.26 ± 1.55 (range 8–77 years) [Table 1] and modal age of 21–30 years who presented with TSCI. They comprised 37 males and 8 females giving a male: female ratio of 4.6:1. There was an average 15 cases/year. Students were mostly affected 11 (24%) followed by farmers 8 (17.8%), traders/businessmen 4 (8.9%), drivers 3 (6.7%), carpenters 3 (6.7%), retirees 2 (4.4%), civil servants 2 (4.4%), and others 12 (26.7%). MVCs were the most common cause of injury 18 (40%) [Table 2].
Head injury was the most common associated injury 16 (35.6%). Others included friction burns 4 (8.9%), chest injury 3 (6.7%), limb fractures 2 (4.4%), urethral injury 1 (2.2%), and pelvic diathesis 1 (2.2%). No associated injury was seen in 18 patients (40%). A large number of the patients presented between 2 and 13 days 34 (75.6%) with associated complications such as pressure sores 14 (31.1%) and burns from traditional setters intervention 1 (2.2%). The cervical spine was the most injured part of the spine accounting for 24 patients (53.3%) followed by thoracic 14 (31.1%) and lumbar spine injuries 7 (15.6%). The cervical spine also accounted for most of the complete injuries at presentation 9 (64.3%) followed by thoracic spine 5 (35.7%).
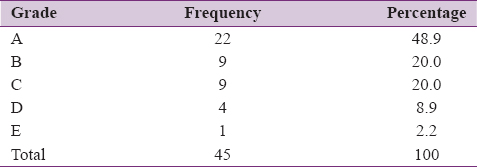
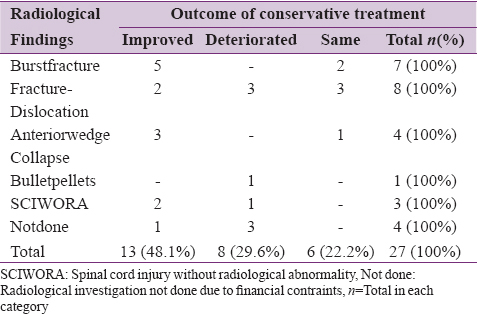
Twenty two patients(48.9%) presented with ASIA Class A [Table 3]. Majority of them presented with quadriplegia 17 (37.8%) and accounted for most of the complete injuries 9 (63.3%) [Table 4]. Most of those that deteriorated had complete injuries [Table 5]. Thirteen out of the 27 patients treated for upto six weeks improved (48.6%), 6 (22.2%) remained the same and 8 (29.6%) deteriorated. Five (71.4%) of those with burst fractures improved [Table 6]. All those that deteriorated eventually died giving a case fatality of 29.6%. Two of the patients were referred while Sixteen were discharged against medical advice earlier than six weeks therefore the result of their treatment was not analysed. The Period of hospitalization ranged from 1-65 days.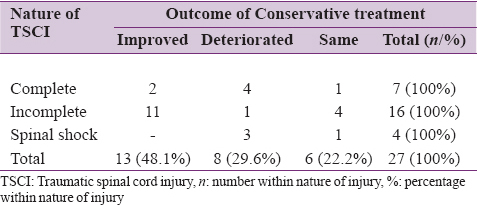 | Table 5: Showing nature of traumatic spinal cord injury at presentation and outcome
Click here to view |
| Discussion | | |
TSCI is on the rise in Makurdi, Nigeria [Table 7]. Our study shows a year on year increase over the 3 years of the study. This rise may be due to a corresponding rise in accidents from dilapidated automobiles on our bad roads as well as a poor driving culture in our environment.[3] Spinal injuries remain an important cause of devastating disability, long hospitalization, and death.[1],[3] This is, especially significant as it affects mainly the young active segment of the population who are crucial to the economy.
The mean age in our study is 33.26 ± 1.55 years which is lower than other studies in Nigeria, by Kawu et al.,[1] Udosen et al.,[8] and Nwankwo et al.[16] where it was 36 years each. However, it is higher than in Turkey, and much less than the USA, where it was found to be 26.8 years and 51 years, respectively.[17] The modal age of 21–30 years was also reported by Obalum et al.[3] in Lagos, Nigeria. This can be explained by the predominance of the students in our study who may engage in long journeys using motor vehicles while traveling for holidays. Fall from trees was the third cumulative cause of TSCI. This could be due to the fact that some children climb trees to get fruits for a free lunch, fetch wood for fire, or just for adventure. The preponderance of the male is due to the high-risk activities of men are involved in as they go about trying to earn a living to fend for their families and dependents. These findings are buttressed by other studies.[18],[19],[20] This further highlights the devastating effect of TSCI on the family and state economy. This is brought about by the loss of productivity following invalidation, death, or disability of these young, vital productive members of the society. The adverse effects of TSCI are not limited to the individual and family alone, it also affects the health facility, society, and national economy.[3]
The most common cause of TSCI was MVC accounting for 40%. This was followed by fall from height 28.8% and motorcycle crash 15.7%. This seems to be the pattern globally because several other studies have similar findings.[2],[3],[17] This may be due to the global increase in high-speed travels coupled with the poor use of protective devices such as helmets and seat belts by our drivers, passengers, palm wine tappers, carpenters walking on skyscrapers, and electricians mounting electric poles in our environment.
There is a growing concern in our region because of the rising incidence of gunshot injuries and gunshot-associated SCI in particular.[21],[22] It accounted for 6.7% of the cases in our study. The injuries are usually complete even if the vertebrae are not fractured. This is due to the cavitation phenomenon associated with these injuries.
Most of the patients presented to the teaching hospital after 2–13 days of injury with 31.1% of them already developing pressure sores. Late presentation is a common feature in our region [1] because of poverty, ignorance, and perhaps distance from tertiary health facilities. Some of the injuries are sustained in remote villages and cheaper alternative treatments such as traditional bone setters are sought before eventually resources are mobilized to come to a tertiary health care. A study in Calabar [8] reported most of the patients (61%) presenting within 24 h, but the study population was small.
Our study showed that majority of the patients had cervical spine injury (53.3%) and accounted for the highest percentage of complete injuries (64.3%). This was followed by thoracic (31.1%) and lumbar (15.6%). This is similar to studies in Lagos [1] and Ilorin,[2] where cervical spine injury accounted for 74.7% and 46.2%, respectively. However, it is at variance with other studies in Calabar [8] and Lagos University Teaching Hospital [3] where the lumbar spine was more common accounting for 43% and 59.9%, respectively. This may be due to high rate of head injuries in our patients. These two injuries are so closely associated that a head-injured patient is assumed to have cervical spine injury until proven otherwise. In our study, 35.6% of the cervical-injured patients also had associated head injury. The ASIA Class A was the most common grade at presentation accounting for 48.9%. This was the finding in similar studies in Lagos,[3] Calabar,[8] and a multicenter study involving three tertiary centers in South Eastern Nigeria,[23] where 91.9%, 71.4%, and 47% were found to be the ASIA Class A at presentation, respectively. This paints a gloomy picture as regards complete recovery because these patients hardly improve by more than one or two steps on this classification. However, efforts should be intensified toward a comprehensive multidisciplinary rehabilitation to make these patients as independent as possible.
The period of hospitalization ranged from 1 to 65 days. This is the shortest range of all the publications on SCI in Nigeria, we reviewed.[1],[2],[8],[16] This may be due to the use of air and water mattresses. A prospective cohort study will need to be done subsequently to ascertain the effect of the mattresses on outcome. All the patients were managed on these devices throughout the period of admission. Even those who had pressure sores healed rapidly. We encouraged the patients to procure an air or water mattress on discharge if they can afford it to prevent pressure sores from developing after discharge from hospital.
Limitation
Some patients were excluded from the study due to inadequate information in the case notes. This is a recognized limitation of retrospective studies.
| Conclusion | | |
TSCI mostly results from road traffic crashes, affects young men, and is associated with the twin tragedy of a significant morbidity and mortality.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Kawu AA, Adebule GT, Gbadegesin SA, Alimi MF, Salami AO. Outcome of conservative treatment of spinal cord injuries in Lagos, Nigeria. Niger J Orthop Trauma 2010;9:21-3.  |
| 2. | Solagberu BA. Spinal cord injuries in Ilorin, Nigeria. West Afr J Med 2002;21:230-2. |
| 3. | Obalum DC, Giwa SO, Adekoya-Cole TO, Enweluzo GO. Profile of spinal injuries in Lagos, Nigeria. Spinal Cord 2009;47:134-7. |
| 4. | Olasode BJ, Komolafe IE, Komolafe M, Olasode OA. Traumatic spinal cord injuries in Ile-Ife, Nigeria, and its environs. Trop Doct 2006;36:181-2. |
| 5. | Umaru H, Ahidjo A. Pattern of spinal cord injury in Maiduguri, North Eastern Nigeria. Niger J Med 2005;14:276-8. |
| 6. | Nwadinigwe CU, Iloabuchi TC, Nwabude IA. Traumatic spinal cord injuries (SCI): A study of 104 cases. Niger J Med 2004;13:161-5. |
| 7. | Igun GO, Obekpa OP, Ugwu BT, Nwadiaro HC. Spinal injuries in the Plateau State, Nigeria. East Afr Med J 1999;76:75-9. |
| 8. | Udosen AM, Ikpeme AI, Ngim NE. A prospective study of spinal cord injury in the University of Calabar Nigeria: A preliminary Report. The Internet Journal of Orthopaedic Surgery. 2007;5:344-7. |
| 9. | Ahidjo KA, Olayinka SA, Ayokunle O, Mustapha AF, Sulaiman GA, Gbolahan AT. Prehospital transport of patients with spinal cord injury in Nigeria. J Spinal Cord Med 2011;34:308-11. |
| 10. | Bouamra O, Wrotchford A, Hollis S, Vail A, Woodford M, Lecky F. Outcome prediction in trauma. Injury 2006;37:1092-7. |
| 11. | Furlan JC, Krassioukov AV, Fehlings MG. The effects of gender on clinical and neurological outcomes after acute cervical spinal cord injury. J Neurotrauma 2005;22:368-81. |
| 12. | Baker SP, O'Neill B, Haddon W Jr., Long WB. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J Trauma 1974;14:187-96. |
| 13. | Coelho DG, Brasil AV, Ferreira NP. Risk factors of neurological lesions in low cervical spine fractures and dislocations. Arq Neuropsiquiatr 2000;58:1030-4. |
| 14. | Gabbe BJ, Cameron PA, Wolfe R. TRISS: Does it get better than this? Acad Emerg Med 2004;11:181-6. |
| 15. | Gabbe BJ, Cameron PA, Wolfe R, Williamson OD, Cameron PA. Predictors of mortality, length of stay and discharge destination in blunt trauma. ANZ J Surg 2005;75:650-6. |
| 16. | Nwankwo OE, Katchy AU. Outcome of a 12-week programme for management of the spinal cord injured with participation of patient's relations at Hilltop Orthopaedic Hospital, Enugu, Nigeria. Spinal Cord 2003;41:129-33. |
| 17. | Selvarajah S, Hammond ER, Haider AH, Abularrage CJ, Becker D, Dhiman N, et al. The burden of acute traumatic spinal cord injury among adults in the United States: An update. J Neurotrauma 2014;31:228-38. |
| 18. | Price C, Makintubee S, Herndon W, Istre GR. Epidemiology of traumatic spinal cord injury and acute hospitalization and rehabilitation charges for spinal cord injuries in Oklahoma, 1988-1990. Am J Epidemiol 1994;139:37-47. |
| 19. | Agarwal P, Upadhyay P, Raja K. A demographic profile of traumatic and non-traumatic spinal injury cases: A hospital-based study from India. Spinal Cord 2007;45:597-602. |
| 20. | Karamehmetoglu SS, Nas K, Karacan I, Sarac AJ, Koyuncu H, Ataoglu S, et al. Traumatic spinal cord injuries in Southeast Turkey: An epidemiological study. Spinal Cord 1997;35:531-3. |
| 21. | Mohammed AZ, Edino ST, Ochicha O, Umar AB. Epidemiology of gunshot injuries in Kano, Nigeria. Niger J Surg Res 2005;7:296-9. |
| 22. | Elachi IC, Yongu WT, Ahachi CN, Onyemaechi NO, Odatuwa-Omagbemi DO, Mue DD. The pattern of civilian gunshot injuries at a University Hospital in North Central Nigeria. IOSR J Dent Med Sci 2015;2:87-90. |
| 23. | Uche EO, Nwankwo OE, Okorie E, Nnezianya I. Cervical spine injury: A ten-year multicenter analysis of evolution of care and risk factors for poor outcome in Southeast Nigeria. Niger J Clin Pract 2015;18:203-8. [ PUBMED]  |
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5], [Table 6], [Table 7]
|









 Search Pubmed for
Search Pubmed for