|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2013 | Volume
: 8
| Issue : 4 | Page : 186-188 |
|
Radiation doses from chest X-ray examinations for pediatrics in some hospitals of Khartoum State
N. O. Alatts, A. A. Abukhiar
Department of Radiology, Faculty of Radiologic Sciences and Nuclear Medicine, Ribat National University, Khartoum, Sudan
| Date of Web Publication | 22-May-2014 |
Correspondence Address:
N. O. Alatts
Faculty of Radiologic Sciences and Nuclear Medicine, Ribat National University, Khartoum
Sudan
  | Check |
DOI: 10.4103/1858-5000.133018 
Introduction: Paediatrics patients deserve special attention because of the higher radiation risks compared with adults. Objective: The purpose of this study is to determine diagnostic reference level through entrance surface dose (ESD) calculations. The overall data consisted of patients doses collected from three major hospitals in Khartoum state. Results: 400 patients were subjected to this study. They are classified into four age groups, 0->1 year, 1->5 years, 5->10 years and 10->15 years old. Anteroposterior (AP) chest X-ray examination is done for them. The ESD calculated using Dose Cal software. The x-ray tube output for each equipment is measured using calibrated ionization chamber (RAD - Check Plus model 06-526). The results obtained are high compared to international diagnostic reference levels for chest. These results will also serve as a base line data for future settings. Keywords: Pediatrics, radiation dose, Sudan, X-ray
How to cite this article:
Alatts NO, Abukhiar AA. Radiation doses from chest X-ray examinations for pediatrics in some hospitals of Khartoum State. Sudan Med Monit 2013;8:186-8 |
| Introduction | |  |
A result of 100 years of research in radiobiology, have shown that radiation can cause biological effects. The biological effects of radiation are either stochastic or deterministic. [1] The former concerns with any dose no matter how small, that the potential to cause harm does exist. [2] If harm occurs the damage generally becomes apparent years after exposure. [3] Probability of effect increases with increasing dose. The latter concerns with the immediate effects that can take place after a certain dose have been exceeded (threshold).
The risk of biological effects manifestation is higher in infants and children due to their young cells. [4] In addition to that as a consequences to their longer life expectation this places an added burden on staff to attain the best possible result every time.
In recent years extensive efforts have been made to reduce the risk of irradiation detriment from all sources of medical radiation including X-rays. [5] Among these effort is the establishment of diagnostic reference levels (DRL's). According to the international commission on radiological protection, the DRL is defined as 'the dose levels in medical radio-diagnostic practices for typical examination for groups of standard-size patients or standard phantom for broadly defined types of equipment. [6] These levels are expected not to be exceeded for standard procedures when good and normal practice is applied'. [7]
This study deals with infants and children undergoing chest X-ray examination. They are grouped according to their ages as follows: 0->1 year, 1->5 years, 5->10 years and 10->15 years old. The chest X-ray is chosen being the most common type of X-ray examination and the projection subject for the study is antero-posterior.
The major motivation of the study is to obtain image quality consistent with the medical imaging task particularly in infants and children by reinforcing As Low As Reasonably Achievable (ALARA) philosophy [8] and to provide guidance and advice on establishment and implementation of DRL's.
The ultimate goal of this work is to evaluate the radiation dose delivered to infants and children patients undergoing chest X-ray examination through determination of entrance surface dose (ESD). In Sudan to the best of our knowledge, the only available dosimetric data for pediatrics are those from the chest examination done in a single department. This work broadens the scale by introducing busy departments in major hospitals in Khartoum state, which show minimum workload of 15-20 patients a day.
The results presented will serve as a base line data needed for deriving DRL's for all kinds of X-ray examination including fluoroscopy, computed tomography and interventional radiography.
| Materials and Methods | | |
Measurements had been taken in a period of 4 months for about 400 patients. Patients was classified into four age groups, 0->1 year, 1->5 years, 5->10 years and 10->15 years.
The dose values were obtained using computer software called DoseCal, which is designed for both adults and children data. This software was developed by radiological protection center of Saint Gorge's hospital, London. ESD was determined from exposure factors recorded at the time of examination. Tube output of all X-ray machines used in this study was measured using calibrated ionization chamber (RAD - Check Plus model 06-526).
| Results | | |
[Table 1] shows distribution of studied groups according to age and sex. [Table 2] gives a summary of maximum, minimum and mean chest dose values for all cases under study and shows the variations in doses for the same age group. [Table 3] shows a summary of maximum, minimum and mean chest dose values for all age groups under study irrespective of sex. [Table 4] gives mean chest dose for the age group 1- >5 years found in this study and similar studies done in some other countries. [9],[10],[11],[12]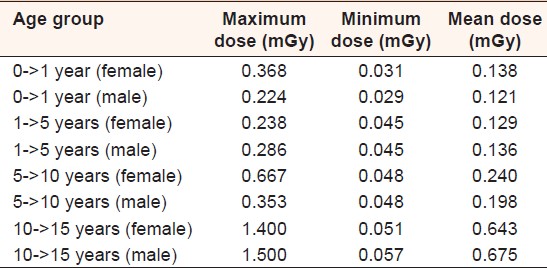 | Table 2: A summery maximum, minimum and mean chest dose values according to age and sex
Click here to view |
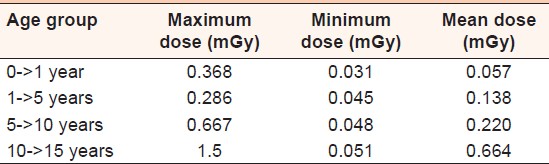 | Table 3: A summary of maximum, minimum, and mean chest dose values for all age groups under study irrespective of sex
Click here to view |
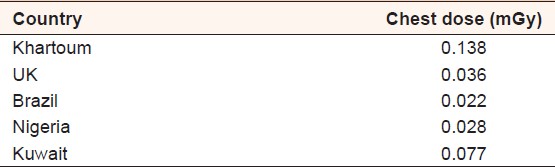 | Table 4: Mean entrance surface dose for chest X-ray for age group 1->5 years in some other countries
Click here to view |
| Discussion | | |
The chest X-ray examination for pediatrics is chosen in this study because it is the most common type of examinations and the selected areas of study are the busiest in Khartoum state in terms of workload. The main aim is to provide baseline for further studies in order to establish local reference dose for each hospital. [Table 2] shows the wide variations between the maximum and minimum dose and the significant differences between sample hospitals. [Table 4] showed the differences between some countries. The ESD presented in our studies is four folds of that in United Kingdom and 6 times of Brazil and double the established ESD in Kuwait. There are multiple reasons for such unacceptably high dose mainly due to the lack of proper collimation. The wide area to be irradiated means higher possibility of cancer induction. The unnecessary wide area covered by the radiation does not impair the quality of the image only but also expose radiosensitive organs like thyroid and deliver more doses to the breast. [3] The second major factor is the low kV and high current-time (mAs) selection. The ideal way to reduce the relative dose is by adopting the high kV technique. [13] Last but not least is the importance of providing specialized X-ray units for children to be operated by highly trained technologists.
| Conclusions | | |
Radiation protection in pediatrics radiology deserves special attention because children are more sensitive to radiation than adults. The results obtained shows:
- Wide dose variation.
- All doses are found to be above the international recommended levels.
- These results could be attributed to performance of equipments and processors, radiographic techniques used in each hospital, film-screen combination, use of grids and or training and skills of the staff.
| Recommendations | | |
- Establishment of Local Reference Dose Levels to be applied to pediatrics radiology departments.
- Importance of quality control programs in medical radiology equipments specially those to be used in pediatrics.
- More attention must be paid for special training for the staff working in pediatrics radiology departments in order to reduce radiation doses and consequently radiation hazards.
- Continuity of such as this study to cover all pediatrics hospitals in Sudan.
| References | | |
| 1. | Hakanen A, Järvinen H, Soimakallio S. Trends in radiology in Finland between 1995 and 2000. Eur Radiol 2003;13:2705-9. 
|
| 2. | Servomaa A, Heikkila M, Ilus T, Parvianen T. Frequency and practice of paediatrics X-ray examinations in Finland 1995. Internal Report. CEC IV - Framework Research Project. 1997.
|
| 3. | International Commission on Radiological Protection. 1990 Recommendations of the International Commission on Radiological Protection. ICRP Publication 60. Oxford: Pergamon Press; 1991.
|
| 4. | Radiation Protection 100, Guidance for Protection of Unborn Children and Infants Irradiated due to Parental Medical Exposures, Directorate-General Environment, Nuclear Safety and Civil Protection European Commission, 1998.
|
| 5. | Montgomery A, Martin CJ. A study of the application of paediatric reference levels. Br J Radiol 2000;73:1083-90.
|
| 6. | Hufton AP, Doyle SM, Carty HM. Digital radiography in paediatrics: Radiation dose considerations and magnitude of possible dose reduction. Br J Radiol 1998;71:186-99.
|
| 7. | Stamm G, Saure HD. Entrance surface dose and its correlation with patient parameters. Radiat Prot Dosimetry 1998;80:235-8.
|
| 8. | McDonald S, Martin CJ, Darragh CL, Graham DT. Dose-area product measurements in paediatric radiography. Br J Radiol 1996;69:318-25.
|
| 9. | Armpilia CI, Fife IA, Croasdale PL. Radiation dose quantities and risk in neonates in a special care baby unit. Br J Radiol 2002;75:590-5.
|
| 10. | Brindhaban A, Al-Khalifah K. Radiation dose to premature infants in neonatal intensive care units in Kuwait. Radiat Prot Dosimetry 2004;111:275-81.
|
| 11. | Freitas MB, Yoshimura EM. An overview of doses to patients and irradiation conditions of diagnostic chest X-ray examinations carried out in hospitals of the City of São Paulo, Brazil. Radiat Prot Dosimetry 2003;103:141-8.
|
| 12. | Ogunseyinde AO, Adeniran SA, Obed RI, Akinlade BI, Ogundare FO. Comparison of entrance surface doses of some X ray examinations with CEC reference doses. Radiat Prot Dosimetry 2002;98:231-4.
|
| 13. | Martin CJ, Farquhar B, Stockdale E, MacDonald S. A study of the relationship between patient dose and size in paediatric radiology. Br J Radiol 1994;67:864-71.
|
[Table 1], [Table 2], [Table 3], [Table 4]
|









 Search Pubmed for
Search Pubmed for