|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2013 | Volume
: 8
| Issue : 4 | Page : 189-193 |
|
Analysis of price discrepancies and its impact on rational use of medicines
Rayan K. Mahmoud1, Hassan M. Ali2
1 Department of Pharmacology, National College for Medical and Technical Studies, Khartoum, Sudan
2 Faculty of Pharmacy, National College for Medical and Technical Studies, Khartoum, Sudan
| Date of Web Publication | 22-May-2014 |
Correspondence Address:
Hassan M. Ali
Faculty of Pharmacy, National College for Medical and Technical Studies, P.O. Box: 3783 Khartoum 11111, Khartoum
Sudan
  | Check |
DOI: 10.4103/1858-5000.133021 
Introduction: The concept of rational use of medicines requires that patients receive quality efficacious medicines appropriate to their needs, in doses that meet their individual requirements, for the adequate period of time and at the lowest cost to them and to the community. Objectives: The objectives of the study were to: 1) Analyze drug price differences between brands included in Sudan Drug Index (2009), 2) compare current drug prices with prices available in the international market (WHO drug price guide 2010), 3) assess the impact of price discrepancy on rational drug use by prescribers, dispensers and patients. Methodology: A descriptive, analytical, one time study was done in Khartoum capital, including 54 drugs selected via a pilot study. Questionnaire was designed to elect the perception, attitude, and behavior of prescribers and dispensers, toward price discrepancy and its impact on rational drug use. Information from patients was taken via a structured interview, using a probability value of 0.07; the sample size was 184 pharmacists, 196 doctors and 196 patients. Result: The discrepancy level was very high in Diclofenac Na 75 mg/3 ml inj with an H/L ratio of 73.7. Drug price comparison with the international guide reveled 92.31% of drug prices included in the study were higher than the guide. The impact of price discrepancy on rational drug use by prescribers, dispensers and patients is confusing, indicating a high degree of irrationality. Conclusion: Price discrepancies haven't been explained neither by the national regulatory authority nor by the local agents. The state of confusion on prescribers, dispensers, and patients would be a source of irrational practice with all its implications on rational use of medicines particularly on the end user having the current scarce financial resources. To ensure availability, accessibility and affordability of medicines establishment of a new drug policy becomes of paramount importance. Keywords: Brands multiplicity, dispensers, patients, prescribers, price discrepancy, rational drug use, Sudan drug index
How to cite this article:
Mahmoud RK, Ali HM. Analysis of price discrepancies and its impact on rational use of medicines. Sudan Med Monit 2013;8:189-93 |
| Introduction | |  |
Access to drugs is a combination of three factors: Availability, affordability and rational use. Rational use of medicines requires that patients receive quality efficacious medicines appropriate to their needs, in doses that meet their individual requirements, for the adequate period of time and at the lowest cost to them and to the community. [1]
In developing countries, the availability of standard quality drugs is a chronic problem. The majority of the population cannot afford the high cost of the available drug therapies and drugs are not rationally used. [1] The rising prices of drugs are a considerable drain on the pockets of the entire population, but it affects the poor most.
The World Health Organization (WHO) Policy Perspective on Medicine (2002) indicates that even when drugs are made available, more than 50% are prescribed, dispensed or sold inappropriately while 50% of the patients fail to take the medicines correctly leading to negative consequences. [2]
Passive privatization, the process by which the private sector share of health care grows rapidly while public health expenditure remains stagnant, has been one more reason for increasing costs of health care and increasing out-of-pocket payment on drugs. [3] The rising prices of drugs in the private sector limit access to drugs for a majority of the population. The impact of increasing prices is not only on individuals and households but as well as on the national health systems.
In most other commodities the market competition acts to regulate prices that are dependent on the costs of raw material, the costs incurred in manufacturing and the dynamics of supply and demand. However, this logic of the market-place does not quite apply to drugs since the consumers do not make the choice on which drug to consume, it is the doctors who make the decision on their behalf. On the other hand, most drug promotion by drug companies is based on branded drugs and their promotion to doctors and pharmacists. [3]
Generic drugs can tremendously increase the availability, affordability and appropriate use of medicines. Price appears to be the real difference between most brands and generic drugs. Generic drugs are held to the same quality standards for safety and performance as the brand names, yet can sell for 30-80% less and in fact on an average, most generic drugs are approximately half the price of their branded counterparts. [3]
In developing countries, studies and data on medicines prices are scanty. Investigational studies of the set prices of medicines are the first stage in developing medicine pricing policies that would ensure affordability.
Sudan is facing major challenges with increasing medicine costs and multiplicity of brands leading to major price discrepancy problems. The study is targeted to evaluate price discrepancy of drugs and its impact on rational drug use.
| Materials and methods | | |
A descriptive, analytical, 1 time study was done in Khartoum capital, including 54 drugs selected via a pilot study, their prices were taken from Sudan Drug Index 2009. A questionnaire was designed to elect the perception, attitude and behavior of prescribers and dispensers, toward price discrepancy and its impact on rational drug use. Information from patients was taken through a structured interview. Using a P - 0.07; the sample size was 184 pharmacists, 196 doctors and 196 patients, selected through a multistage sampling method (cluster and simple random sampling). Drug prices were analyzed using Excel. Questionnaires and interviews were analyzed by a Statistical Package for the Social Sciences 16 program (SPSS Inc., 233s. Wacker Drive Chicago, II. 60606-6412 USA).
More than 189 products from the sampled drugs were included in the study. All brands of drugs were classified based on their strength and type of dosage form in which they are formulated. Prices on the index were collected and converted to a uniform currency (United States dollar). Unit price were calculated by dividing the package price by the package size. A high low ratio (H/L) was calculated to select drugs for graphic representation of price discrepancy, where for each drug only the dosage forms with an H/L ratio of (≥9) were taken. The criteria of selection was determined based on a pilot study, which was done by asking citizens with moderate income about how much they are ready to pay for a drug known to have different brands. Most of them said they'll pay a maximum of 9 times that of the lowest price brand. The median prices were obtained for each pharmaceutical dosage form. These median prices were compared with the international reference price, using the international drug price indicator guide (WHO drug price guide 2010). Comparing drug prices on the buyer comparison form, with the prices collected from Sudan Drug Index (Cost Insurance and Freight prices) and hence there was no need for price adjustment. The total number of dosage forms included in the study and were on the buyer comparison form were 117 products, from 47drugs.
| Results | | |
The discrepancy level varied significantly with each product, ranging from very high (e.g., Diclofenac Na 75 mg/3 ml injection H/L ratio of 73.7) to very low and almost no discrepancy at all for the single branded dosage form(s). Drug price comparison with the international guide revealed that 92.31% of drug prices included in the study were higher than the guide. The net conclusion for the impact of price discrepancy on rational drug use by prescribers, dispensers and patients is confusion and a high degree of irrationality.
The analysis of drug price differences between brands included in Sudan drug index (2009)
The discrepancy level was expressed by an H/L ratio for all 36 drugs [Table 1]. Losartan K 25 mg tablet showed the lowest H/L ratio of 9, while Diclofenac Na 75/3 ml injection showed the highest H/L ratio of 73.7 [Figure 1].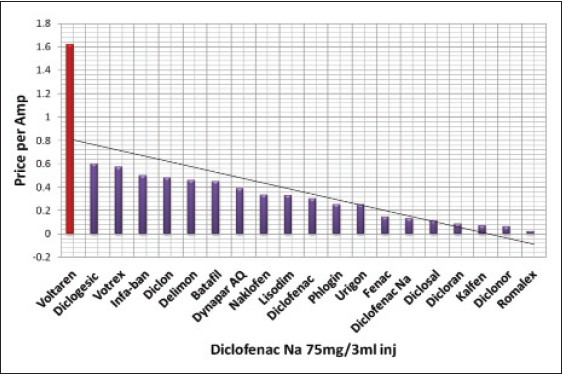 | Figure 1: Price discrepancy of 20 brands of Diclofenac Na 75 mg/3 ml injection. The red column is the originator brand price
Click here to view |
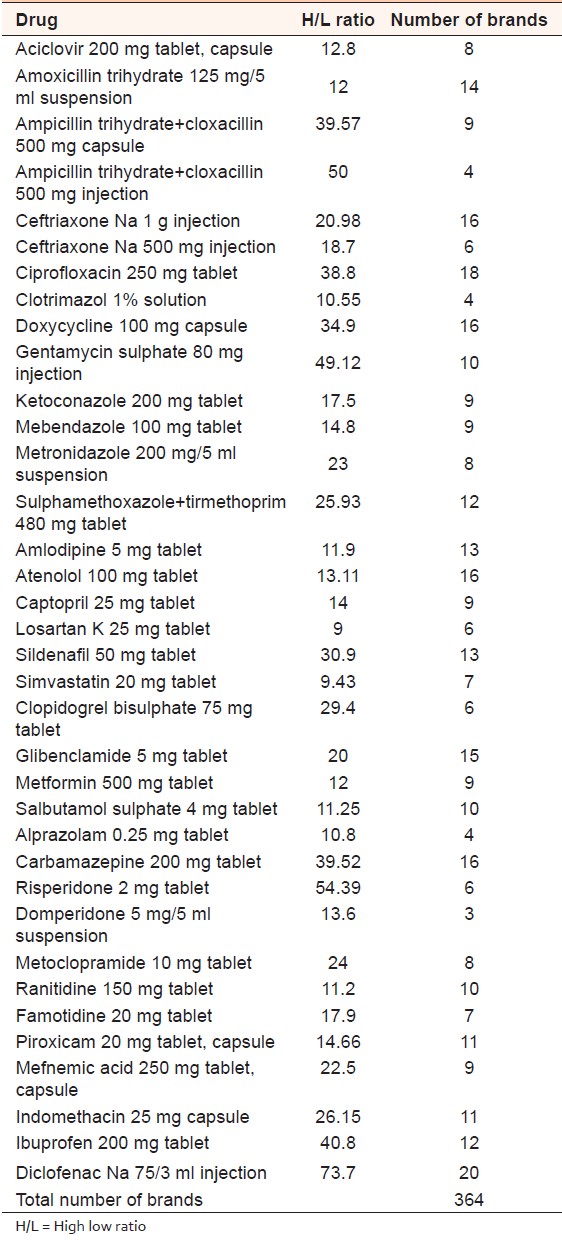 | Table 1: The degree of discrepancy among brands expressed by a (H/L ratio) and number of brands available on each dosage form
Click here to view |
The comparison between current drug prices and prices available in the international market (WHO drug price guide 2010)
Drug products (117) included in the comparison were classified according to their pharmacological group into eight subgroups. The median price of antibiotics, anti-hypertensives, lipid lowering agents, bronchodilators, gastrointestinal tract drugs and oral hypoglycemics were 4.93, 7.47, 6.5, 8.698, 4.61 and 5.12 respectively higher than the international guide.
Antipsychotics prices were 3.09 higher than the international guide; except for Carbamazepine 100 mg/5 ml suspension, Risperidone 2 mg tablet and Diazepam 10 mg tablet prices which were lower than the international price.
Analgesic and anti-inflammatory drugs prices were 3.09 higher than the international guide except for Diclofenac Na 0.1% ophthalmic drops price which was lower than the guide.
The impact of price discrepancy on rational drug use by prescribers, dispensers and patients
Most participating doctors (48%) reported using standard treatment guidelines as their source of information, 47.87% of them were house officers. Whereas 22.4% use the national list of essential medicines, 12.8% get their information from medical representatives, 9.2% use medical journals and 7.7% get their information from the internet.
87% of dispensers think that observed price discrepancies are explainable, whereas only 13% think not. The underlining reasons given include:
- Different manufacturing countries, 41.3%.
- Different shipping and transportation charges, 17.9%.
- Current hard currency fluctuations, 17.4% and,
- 10.3% due to different costs of packaging materials used.
Almost 78.8% of dispensers believe that frequent variation in drug prices affects them while 21.2% doesn't. The impact of price discrepancy on dispensers: 35.9% found it was difficult to deal with, 35.3% were confused. In total, 71.2% are negatively affected by price discrepancy.
Responsibility of price discrepancy from the dispenser's point of view: 45.7% of the dispensers relate the responsibility of price discrepancy to the National Medicine and Poisons Board. [Figure 2].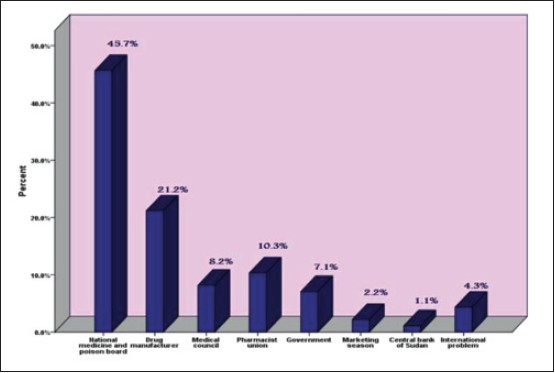 | Figure 2: The responsibility of price discrepancy from the dispenser's point of view
Click here to view |
The attributes of the patients included in the study: Male 51%, female 49%, 59.2% married, 10.7% illiterate and 34.2% with a bachelor degree. The selection of the sample size being limited to Khartoum state is typical of this urban community.
| Discussion | | |
Analysis of drug price differences between brands included in Sudan drug index (2009)
The discrepancy problem for over the counter medications is of lesser impact compared to the situation of prescribed-life saving drugs.
The treatment of chronic conditions such as (asthma, diabetes and cardiovascular disease) often requires a combination of medicines, the cost of which is expected to be even more unaffordable considering their respective high prices. The lifelong use of such medications increases the financial burden for the patients specially the poor ones.
Multiplicity of brands was very high for antibiotics, which is often the major contributing factor for their irrational use, misuse and the emergence of resistance problems.
The originator brand was the highest in cost compared with its generics, e.g., Diclofenac Na 75/3 ml injection, the price of Voltaren ($1.622/Amp) was 73 times that of Romalex ($0.022/Amp). Voltaren price was 2.7 times that of the medium priced generic (Diclogesic).
Comparison between current drug prices and prices available in the international market (WHO drug price guide 2010)
Among all 117 products studied the prices of 108 of them (92.31%) were higher than those of the guide indicating that less expensive sources are still available.
The prices of nine drugs which represent 7.69% of total drugs included in the study were lower than those of the international guide; this might be attributed to a limited market demand and/or different manufacturing procedures/materials used.
These results of these comparisons in our opinion constitute sufficient evidence to take them as indicators to warrant further investigations at the administrative, managerial and regulatory levels of the national health authorities.
The impact of price discrepancy on rational drug use by prescribers, dispensers and patients
When prescribers are asked the question how they choose a product from different brands of the same generic, 46.4% said they prescribe based on patient socio-economic status, 17.3% go for the cheaper products, 6.1% prescribe products that suit the patients to ensure their compliance. They assume that prescribing expensive drugs for low socioeconomic status patients is a major contributing factor to non-compliance and therapeutic failure. Female prescribers (50.9%) are influenced by the patient socio-economic status, expectedly feeling-influenced!
Prescribing based on prescribers clinical experience constitutes 30.1%. However, a valid justification for this was not provided since they didn't try all brands available. Statistical records showing the validity of their selection were lacking.
Others, 21.9% prescribe based on pharmaceutical companies ranking, claiming their products to be the most effective ones (big companies always make good drugs!!!!) but it's more likely a result of manufacturer's promotional activity (pressure!!!).
Only 1.5% (3 out of 196 prescribers) prescribes by generic names being believers of the rational prescribing concept, (i.e., not influenced by the prevalence of brand phobia epidemic).
From all participating doctors, 59.7% have neither justified their choice for the drugs nor have stated the underlying reason(s) for that.
Prescribers accepting the observed pattern of price discrepancy were 64.3%. The brand multiplicity in their view offers them greater choices for their selection.
The impact of price discrepancy on prescribers
Nearly 22.4% found it difficult to deal with specially the unpredictable increase in drug prices and 19.9% were confused. The net result of 42.3% is high enough to be considered an irrational practice.
Public sector pharmacists have no choice but to follow what the medical doctors prescribe, in line with the hospital administrative and regulatory guidelines, which allow brand prescribing. However, this prescribing practice is bound to nullify the privilege of the public over private sector services.
Pharmacists dispensing of prescription drugs
Nearly 33.7% justified this dispensing practice as selecting the most effective product, an argument that lacks any scientific justification in conflict with the National Regulatory Authorities where brands are registered as equal with respect to efficacy and safety, but neglecting cost.
National Medicines and Poisons Board (NMPB) adopts the British National Formulary and Food and Drug Administration orange book registration guidelines as their reference however the NMPB practice is neither in line with the situation in UK nor that in USA where brand prescribing is very much limited to certain products e.g., life-saving drugs, narrow therapeutic index products.
Patients choice of products
Almost 11.7% they go for the cheapest where as 15.3% they prefer the expensive products based on the believe that expensive products are the effective ones, a behavior closer to our Sudanese culture. 34.2% of patients accept what their doctor prescribes. On the other hand 31.1% they purchase the products they can afford to pay for and 7.7% of the patients rely on the dispensers choice.
Assessment of affordability elements in relation to continuation of their respective therapy indicated that 64.3% of patients continue therapy regardless of cost, while 35.7% cease their treatment due to un affordability. Lack of access to health facilities and extremely high prices leads patients to discontinue their treatments and look for other alternatives e.g., herbal medicines.
Most patients were not aware that most expensive brands have cheaper alternatives (52%), while 48% were aware of it 33.2% of the patients accept the observed price discrepancy and 66.8% were against it.
How do patients view drug prices discrepancy?
Nearly 40.3% of patients were confused, 28.1% are unconfident of the drugs they are using and 12.2% described the situation as a discriminative attitude and practice. This situation has serious implications especially when dealing with psychotropic medicines where the patient mental state is of paramount importance in the success of therapy.
The unacceptability of the observed drug price discrepancy is becoming a growing concern nationwide.
| Conclusion | | |
The study has shown high degree of price fluctuation among brands with life-saving drugs having highest degree of discrepancy level.
The products included in the study demonstrated a significant prices difference compared with those of the international guide where the prices of 92.31% of these drugs were higher than those of the guide.
To the best of our knowledge the observed price discrepancies have not been explained neither by the national regulatory authorities nor by the local agents. Moreover, the underlining reasons behind the discrepancies have not been explained neither by the public nor by the private sector suppliers. This situation reflects to a greater extent an irrational practice. The inter-brand price differences were often related to the manufacturers countries of origin i.e., prices from the industrialized countries have often been greater than those from the developed and under-developed countries. However, the inter-brand differences between the developing countries manufacturers are in our view neither justified nor explained.
The brands multiplicities coupled with the price discrepancy have led to state of confusion for the three parties involved in the drug use chain, the prescriber, the dispenser and the patient. The state of confusion observed is expected to be a major cause of irrational drug use and the implications of this practice is very much expected to question the effectiveness and safety of drug therapy as well as to its consequent financial impact on the end users particularly at the present time. Sudan national economy is currently facing serious problems with steadily growing scarcity of its major resources.
| References | | |
| 1. | Amanda Le Grand, Hans V Hogerzeil, Flora M Haaijer- Ruskamp, Intervention research in rational drug use of drugs: a review, Oxford university press 1999, health policy and planning;14(2):89-102. 
|
| 2. | W.H.O. Promoting Rational Use of Medicines: Core Components. W.H.O Policy Perspectives on Medicines. WHO headquarter, Geneva, Switzerland:; 2002. p. 1.
|
| 3. | Sundram S. Promoting Rational Drug use Need for an NRHM Sub-mission. Published by national health system resource center NHSRC India, August, 2009.
|
[Figure 1], [Figure 2]
[Table 1]
|









 Search Pubmed for
Search Pubmed for