|
 
 |
| REVIEW ARTICLE |
|
| Year : 2014 | Volume
: 9
| Issue : 3 | Page : 127-131 |
|
Identification of varied Sudanese infants ages (at birth, day 4, and 8 weeks) by determination of ossification pattern in the anterior skull base using computed tomography scan (A qualitative postmortem study)
Tarig Gasim Mohamed Alarabi1, Ogail Elnour Mohamed Swar Eldahab2
1 Department of Anatomy and Embryology, Faculty of Medicine, International University of Africa, Sudan
2 Central Morgue, Bashair Teaching Hospital, Ministry of Health, Khartoum State, Sudan
| Date of Web Publication | 22-Jan-2015 |
Correspondence Address:
Tarig Gasim Mohamed Alarabi
Department of Anatomy and Embryology, Faculty of Medicine, International University of Africa, Africa Street, P.O. Box 2469, Khartoum
Sudan
  | Check |
DOI: 10.4103/1858-5000.149838 
Medico legally this study identify certain Sudanese infants ages (at birth, day 4, and 8 weeks) through description of ossification pattern in the anterior skull base using computed tomography (CT) scan. Also, it is describing the normal anatomical pattern of ossification. So this study will explain and reveals the Sudanese own skull base bony print. Total number of selected cases for study are 12 died children admitted to Mortuary of Khartoum between July\2011 and November\2011, and all cases of known age, sex and nationality (Sudanese) according to police records, confirmed medico legally by evaluation of external signs of live. All cases were examined in Khartoum teaching hospital at January\2012 that explained the skull base development and ossification by direct coronal CT scans, 1 mm and wide window (bone) settings of Para Nasal Sinuses (PNS) protocol. The used CT scan machine is TOSHIBA-Asteion. The observations of day 1, 4 and 8 weeks explained that each determined age has its own skull base bony pattern. Also observations of those ages revealed that the development of the forming parts of skull base which include orbital plates and its extension over lateral ethmoidal air cells, roof of ethmoid complex, cribriform plate, perpendicular plate of ethmoid and ethmoidal air cells was progressively increasing with age except; the perpendicular plate of ethmoid bone which doesn't meet the vomer in the posterior septum at any of these certain ages although vomer was ossified at those varied ages. And the Crista galli neither ossified nor fused with ethmoidal labyrinths at all. Also, the Ethmoidal air cells have never been extended above the plane of the cribriform plate. Observed ages and patterns of ossification was different somewhat from that reported in prior radiologic and anatomic studies in the ethmoidal complex and its extension over the cribriform plate of ethmoid bone also in the crista, galli which was seen ossified as early as 2 months of age in previous study.
Keywords: Skull anatomy, skull base, skull, growth and development
How to cite this article:
Alarabi TG, Eldahab OE. Identification of varied Sudanese infants ages (at birth, day 4, and 8 weeks) by determination of ossification pattern in the anterior skull base using computed tomography scan (A qualitative postmortem study). Sudan Med Monit 2014;9:127-31 |
How to cite this URL:
Alarabi TG, Eldahab OE. Identification of varied Sudanese infants ages (at birth, day 4, and 8 weeks) by determination of ossification pattern in the anterior skull base using computed tomography scan (A qualitative postmortem study). Sudan Med Monit [serial online] 2014 [cited 2018 Feb 24];9:127-31. Available from: http://www.sudanmedicalmonitor.org/text.asp?2014/9/3/127/149838 |
| Introduction and background | |  |
From a practical standpoint, an understanding of the appearance of the normal developing anterior skull base is important for several reasons. First, it prevents misinterpreting normal development for a pathologic state. Second, it reveals the limitations of computed tomography (CT) in evaluations of the anterior skull base in young patients. Finally, it may allow further insight into the underlying mechanism for the development of anomalies of the anterior skull base. The precise sequence of ossification and the CT appearance of the anterior skull base during the first 2 months of life are the subjects of this study. An understanding of the development of the anterior skull base begins with a brief review of skull base embryology. The skull can be divided into two parts: The neurocranium, which forms a protective case around the brain, and the viscerocranium, which forms the skeleton of the face. The neurocranium is the most conveniently divided into two portions: (a) The membranous part, consisting of flat bones, which surround the brain as a vault; and (b) the cartilaginous part, or chondrocranium, which forms bones of the base of the skull. The membranous neurocranium portion of the skull is derived from neural crest cells and paraxial mesoderm. Mesenchyme from these two sources invests the brain and undergoes membranous ossification. The result is the formation of a number of flat, membranous bones that are characterized by the presence of needle-like bone spicules. [1] These spicules progressively radiate from primary ossification centers toward the periphery. [1] With further growth during fetal and postnatal life, membranous bones enlarge by apposition of new layers on the outer surface and by simultaneous osteoclastic resorption from the inside. The cartilaginous neurocranium or chondrocranium of the skull initially consists of a number of separate cartilages. Those that lie in front of the rostral limit of the notochord, which ends at the level of the pituitary gland in the center of the sella turcica, are derived from neural crest cells. They form the prechordal chondrocranium. Those that lie posterior to this limit arise from paraxial mesoderm and form the chordal chondrocranium. The development begins as a mesenchymal condensation along sides and in front of the notochord during the fifth and sixth fetal weeks. [2],[3] The chondrification of this mesenchyme occurs around the seventh fetal week. [4] The base of the skull is formed when these cartilages fuse and ossify by endochondral ossification. The base of the occipital bone is formed by the parachordal cartilage and the bodies of three occipital sclerotomes. Rostral to the occipital base plate is the hypophyseal cartilages and trabeculae cranii. These cartilages soon fuse to form the body of the sphenoid and ethmoid, respectively. So during the second fetal month, enchondral ossification of the chondrocranium forms the basioccipital, basisphenoidal, and presphenoidal centers. [3] Anterior to these centers, portions of the presphenoidal cartilage give rise to the mesoethmoidal cartilage, which forms the central structures of the anterior skull base, the perpendicular plate of the ethmoid bone, and the crista galli. In this manner, an elongated median plate of cartilage extending from the nasal region to the anterior border of the foramen magnum forms. A number of other mesenchymal condensations arises on either side of the median plate. The most rostral, the ala orbitalis, forms the lesser wing of the sphenoid bone. Caudally, it is followed by the ala temporalis, which gives rise to the greater wing of the sphenoid. The third component, the periotic capsule, gives rise to the petrous and mastoid parts of the temporal bone. These components later fuse with the median plate and with each other, except for openings through which cranial nerves leave the skull. [5]
We were suggested the anterior base of skull to be the target of our study, because there were many died infants came to the mortuary with amputated parts or limbs either by animals or due to complete analysis of body, or due to any kind of environmental challenges that the refused infant can been exposed to it. Over all that, we know that the base of the skull is the most protected part of the skull, and it is surrounded anatomically by different soft tissues and bones.
Objectives
- Medico legally this study identify the age of died infants who enter to the mortuary with a large numbers
- It is describing the normal anatomical pattern of ossification, and this is important to understand the other abnormal one
- So this study will explains and reveal the Sudanese own skull base bony print
- This study aimed to determine and to classify the ossification centers of the skull base
- The understanding of the age of died newborn makes the dissection report more accurate and highly powerful.
Review of literature
At birth, the anterior skull base consists primarily of the central, unossified cartilage of the perpendicular plate of the ethmoid bone and crista galli, a largely unossified roof of the nasal cavity, and partially ossified ethmoidal labyrinths. [6]
The ossification of the anterior skull base was very limited in the newborn but developed rapidly during the first 6 months. All subjects younger than 2 months old, had areas of partial ossification, and none had complete ossification. Also at birth, the frontal bones were well ossified and extended to the medial edge of the orbit. The ossification of the cribriform plate began in the region of the vertical attachments of the superior and middle turbinates and spread along the surface of the cribriform plate to reach the crista galli at approximately 2 months of age. [7]
Also at day 1 of birth, the outline of the crista galli is just barely visible, and there is very early ossification of the roof of the ethmoidal labyrinth, also some ethmoidal air cells have formed. And the orbital plates of the frontal bones extend to the lateral margin of the ethmoidal complex. [7]
The Ossification of the crista galli began in all subjects between 1 st and 2 nd months of age. And the Ossification of the perpendicular plate of the ethmoid bone approximately paralleled that of the crista galli. The perpendicular plate of the ethmoid bone was also unossified at birth, and its ossification began as early as 2 months of age. [7]
For the fovea ethmoidalis, there was no extension of ethmoidal air cells above the cribriform plate in subjects 2 months of age and younger. [7]
| Materials and methods | | |
The total number of the selected cases for the study are 12 died children admitted to the mortuary of khartoum between July\2011 and November\2011, and all cases of known age, sex and nationality (Sudanese) according to police records, assisted by the medico legal examination which was depended on the evaluation of external signs of live, which include the: The changes around the base of umbilicus (Hyperemia - Indicates for day 1 Ulceration - Indicates for day 2, Stump - Indicates for 1-week and Formed umbilicus - Indicates for 2 weeks), desquamation of skin and macerations. [8] Also in reviewing the cases, we excluded any children who had metabolic and developmental abnormalities like microcephaly, macrocephaly, or any other condition that could conceivably affect development of the anterior skull base. 16.7% of cases were not passed the criteria of the study. In the remaining 83.3% of cases (60% female and 40% male) of four varied age durations were included in this study as follow: 40% children at day 1, 30% children at day 4 and 30% children at 8 weeks). All cases were examined by coronal CT scans in Khartoum teaching hospital at January\2012 which reviewed the skull base development and ossification with direct coronal CT scans, with 1 mm and wide window (bone) settings of PNS protocol. The used CT scan machine is TOSHIBA - Asteion trade mark. Additional parameters were taken from each case to form the general data which include: Weight, Length, Head circumference, Biparietal length and the Nasal septum length (N.B: CT scan was also used in measurement of last two parameters). [9]
| Results | | |
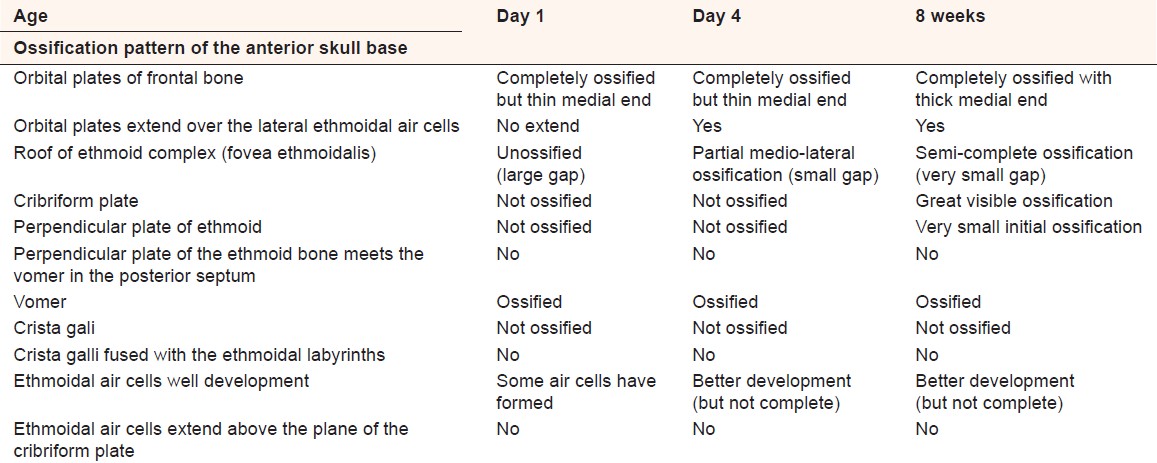
The results could be detailed [Table 1] [Table 2] [Table 3].
| Discussio | | |
It is important to understand the appearance of the developing anterior skull base to avoid interpretive errors in this complex region. Prior, the anatomical studies have described the embryologic and fetal development of the anterior skull base in detail, but few studies have detailed the postnatal development and postmortem pattern of ossification of the anterior skull base as in infants and young children. Our results demonstrate that as a child matures, ossification of the anterior skull base proceeds in a fairly constant pattern, and any age duration has own ossification pattern as follow:
The observations of day 1 revealed that the orbital plates of the frontal bone were completely ossified and had a thin medial end but no extension over the lateral ethmoidal air cells. The roof of ethmoid complex (Fovea ethmoidalis) was not ossified and characterized by large (not ossified) gap. Although the vomer was ossified, it cannot meet the perpendicular plate of the ethmoid in the posterior nasal septum because the later was not ossified. The Crista galli also was not ossified and not fused with the ethmoidal labyrinths. We also observed some of the Ethmoidal air cells were formed, but it has no extension above the plane of the cribriform plate. The cribriform plate was not ossified [Figure 1].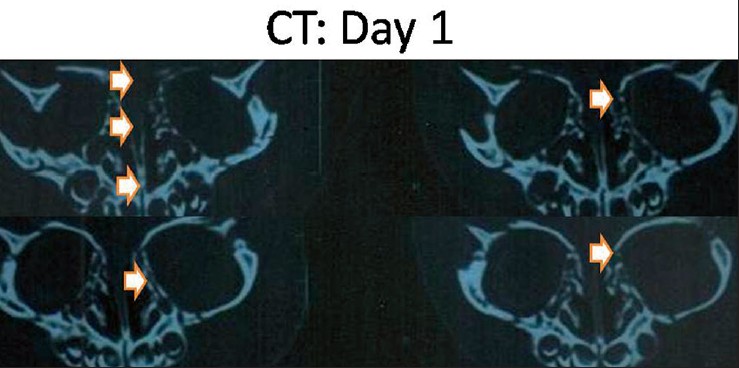 | Figure 1: Coronal computed tomography bone scan of skull base for day 1 infant revealed that orbital plates of frontal bone were completely ossified and has a thin medial end but no extension over the lateral ethmoidal air cells. Roof of ethmoid complex was not ossified and characterized by large not ossified gap. Vomer was ossified, but it cannot meet the perpendicular plate of the ethmoid in the posterior nasal septum. Crista galli also was not ossified and not fused with the ethmoidal labyrinths. Ethmoidal air cells were formed, but it has no extension above the plane of the cribriform plate. Cribriform plate was not ossified
Click here to view |
The observations of day 4 revealed that the orbital plates of the frontal bone were completely ossified and had a thin medial end extend over the lateral ethmoidal air cells. The roof of ethmoid complex (Fovea ethmoidalis) was ossified partially with a small gap between the ossified medial and lateral extensions. Also (like day 1) and although the vomer was ossified, it cannot meet the perpendicular plate of the ethmoid in the posterior nasal septum because the later was not ossified. The Crista galli also like day 1 was not been ossified yet, so it was not fused with the ethmoidal labyrinths. We also observed some of the ethmoidal air cells were formed and developed better than before (day 1), but it has no extension above the plane of the cribriform plate. The cribriform plate was not ossified [Figure 2].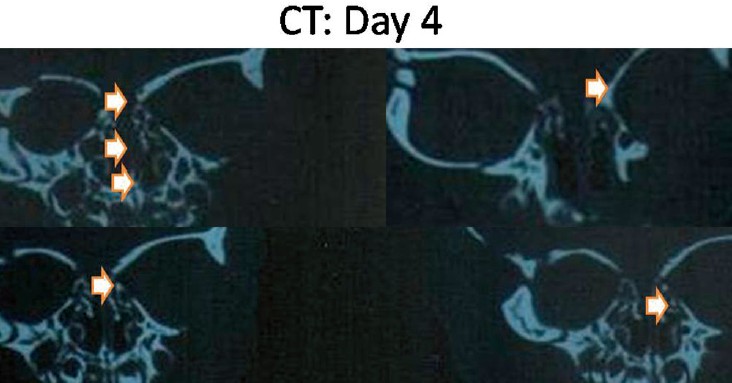 | Figure 2: Coronal computed tomography bone scan of skull base for day 4 infant revealed that orbital plates of the frontal bone was completely ossified and had a thin medial end extend over the lateral ethmoidal cells. Roof of ethmoid complex was ossified partially with gap between the ossified medial and lateral extensions. Vomer was ossified, but not meet perpendicular plate of the ethmoid in posterior nasal septum. Crista galli was not been ossified yet, so it was not fused with the ethmoidal labyrinths. Ethmoidal air cells were developed. No extension above the plane of the cribriform plate. The cribriform plate was not ossified
Click here to view |
The observations of week 8 ossification pattern revealed that the orbital plates of frontal bone were completely ossified and has a thick medial end (not thin like day 1 and day 4) but in this age of live, there was extension of that plates over the lateral ethmoidal air cells. The roof of ethmoid complex (Fovea ethmoidalis) was ossified partially with very small gap between the ossified medial and lateral extensions. Although the vomer was ossified, but it cannot meet the perpendicular plate of the ethmoid in the posterior nasal septum because the later was not ossified till this age. The Crista galli also was not ossified and not fused with the ethmoidal labyrinths. The majority of the cribriform plate was ossified. We also observed some of the ethmoidal air cells were formed and developed better than previous reported ages [Figure 3], but it has no extension above the plane of the cribriform plate although a previous study revealed that the extension of cells over the level of cribriform plate is starts in this age. [7]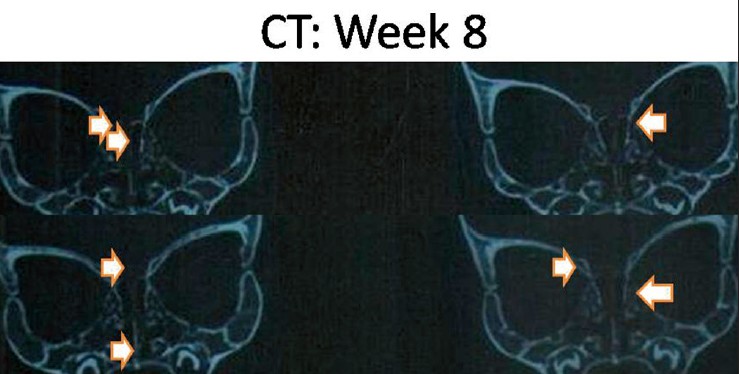 | Figure 3: Coronal computed tomography bone scan of skull base for week 8 ossification pattern revealed that orbital plates were completely ossified with thick medial end there was an extension of that plates over the lateral ethmoidal cells. Roof of ethmoid complex was ossified partially with very small gap between the ossified medial and lateral extensions. Vomer was ossified but did not meet perpendicular plate of the ethmoid in posterior nasal septum. Crista galli not ossified and not fused with the ethmoidal labyrinths. Cribriform plate was ossified. Ethmoidal cells were developed no extension above plane of the cribriform
Click here to view |
| Conclusion | | |
The observed ages and patterns of ossification was different somewhat from that reported in prior radiologic and anatomic studies, with the ethmoidal complex and its extension over the cribriform plate of ethmoid bone, also in the crista galli, which was seen ossified as early as 2 months of age in previous study. The understanding of the ossification pattern of the anterior skull base is important for identification and determination of actual and real age, which is markedly clear between the three studied ages. And the study was summarized these differences as follow: The orbital plates of frontal bone is completely ossified but it has thin medial end in day 1 and day 4, but it is completely ossified with thick medial end in 8 weeks. Also, the extension of orbital plates over the lateral ethmoidal air cells did not occur in day 1 but it occurred in day 4 and week 8. Also the roof of ethmoid complex (Fovea ethmoidalis) was varied from not ossified with large gap in day 1, to partial ossification with small gap in day 4, and semi-complete ossification with very small (slit like) gap in 8 weeks. Also, the perpendicular plate of the ethmoid was not ossified in day 1 and day 4, but it has a very small initial ossification in 8 weeks. Also, the cribriform plate of the ethmoid was not ossified in day 1 and day 4, but it has a great ossification in 8 weeks. Finally, and from the observation of the Ethmoidal air cells, its development was increased by the increasing of age, and that is why it is better in week 8> day 1 and day 4.
| References | | |
| 1. | Sadler TW. Langman's Medical Embryology. 9 th ed. United State of America: Lippincott Williams and Wilkins; 2003. p. 171-6.  |
| 2. | Nadich TP, Zimmerman RA, Bilaniuk LT. Midface: Embryology and congenital lesions. In: Som PM, Curtin HD, editors. Head and Neck Imaging. 3 rd ed. St Louis, Mo: Mosby-Year Book; 1996. p. 17-22. |
| 3. | Sperber GH. The cranial base. In: Craniofacial Embryology. 2 nd ed. Dorchester, England: Wright; 1976. p. 78-87. |
| 4. | Hamilton WJ, Mossman HW. Skeletal system. In: Human Embryology. Baltimore, Md: Williams and Wilkins; 1972. p. 532-40. |
| 5. | Moore KL. The skeletal system. In: The Developing Human: Clinically Oriented Embryology. 4 th ed. Philadelphia, Pa: Saunders; 1988. p. 340-3. |
| 6. | Scott JH. The cartilage of the nasal septum (a contribution to the study of facial growth). Br Dent J 1953;95:37-43. |
| 7. | Belden CJ, Mancuso AA, Kotzur IM. The developing anterior skull base: CT appearance from birth to 2 years of age. AJNR Am J Neuroradiol 1997;18:811-8. |
| 8. | Ogail ES, Sherien SM. A Guide to the Essential of Forensic Medicine. 1 st ed. Cairo, Egypt: Tabarak Press; 2007. p. 171-7. |
| 9. | Butler P, Mitchell AW, Harold E. Applied Radiological Anatomy. Cambridge, United Kingdom: Cambridge University Press; 2006; 2006. p. 17-60. |
[Figure 1], [Figure 2], [Figure 3]
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for