|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2016 | Volume
: 4
| Issue : 2 | Page : 75-78 |
|
Prevalence of simian, Suwon, and Sydney creases in acquired idiopathic blindness in some selected schools for the blind in Nigeria
John Nwolim Paul, EA Osunwoke, CW Paul
Department of Human Anatomy, Faculty of Basic Medical Sciences, College of Health Sciences, University of Port Harcourt, Port Harcourt, Nigeria
| Date of Web Publication | 18-Apr-2017 |
Correspondence Address:
John Nwolim Paul
Department of Human Anatomy, Faculty of Basic Medical Sciences, College of Health Sciences, University of Port Harcourt, Port Harcourt
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2315-7992.204679

Background: The study of palmar flexion creases such as simian, Suwon, and Sydney creases is important since they have strong medical implications. Aim: This study was carried out to determine the prevalence of simian, Suwon, and Sydney creases in acquired idiopathic blindness. Materials and Methods: A total of 72 (36 blind and 36 nonblind) participants were recruited for the study that comprised 22 blind male and 14 blind female participants, 18 male and 18 female nonblind participants. The sampling technique used was convenience purposive sampling. Fingerprints and toeprints were obtained using print. Results: The prevalence of palmar creases in blind and nonblind male and female participants showed that the blind participants had 0% prevalence of simian crease, 3.8% prevalence of Suwon, and 0.6% prevalence of Sydney crease, whereas the nonblind participants have 0% prevalence of the creases. In the female blind participants, there was 0% prevalence of simian crease, 1.2% prevalence of Suwon, and 0.6% prevalence of Sydney crease, whereas the nonblind participants have 0% prevalence of the creases. The total prevalence of palmar creases of the blind and nonblind participants was shown, and the simian crease had 0.0% prevalence in the blind and in the nonblind participants. Suwon crease had 2.8% prevalence in the blind and 0.8% in the nonblind participants. Sydney crease had 0.6% prevalence in the blind, but 0.0% prevalence in the nonblind participants. Comparison of the prevalence of the Suwon and Sydney creases in the blind and nonblind was shown to be statistically nonsignificant (P > 0.05), whereas it was significant for simian crease on comparison with the blind and nonblind (P < 0.05). Conclusion: The study has shown that there is no significant difference in the prevalence of Suwon and Sydney crease (P < 0.05), whereas there is a significant difference in the simian crease between the blind and nonblind compared. This study has provided information on the prevalence of palmar creases in people with idiopathic blindness and the nonblind people in Nigeria and by extension the Sub-Saharan Africa.
Keywords: Acquired, idiopathic blindness, Nigeria
How to cite this article:
Paul JN, Osunwoke E A, Paul C W. Prevalence of simian, Suwon, and Sydney creases in acquired idiopathic blindness in some selected schools for the blind in Nigeria. Ann Bioanthropol 2016;4:75-8 |
How to cite this URL:
Paul JN, Osunwoke E A, Paul C W. Prevalence of simian, Suwon, and Sydney creases in acquired idiopathic blindness in some selected schools for the blind in Nigeria. Ann Bioanthropol [serial online] 2016 [cited 2017 Apr 28];4:75-8. Available from: http://www.bioanthrojournal.org/text.asp?2016/4/2/75/204679 |
| Introduction | |  |
There are lines in the palm known as creases or palmar creases.[1] The most common variations can be described with three simple mathematical rules, PIC Model. The PIC model describes 21 types for the primary palmar lines (12 basic types with 5 types that can manifest in different forms). The two most important lines are simian and Sydney lines.[1],[2] Simian Crease: usually, the human palm of the hand is featured with three strong major lines; in medical science, these are often referred to as palmar flexion creases.[1],[2] The lines involved are known as life line (radial longitudinal crease), head line (proximal transverse crease), and heart line (distal transverse crease). An important variant is found when both lines are “replaced” by one single line which extends the full palm, this single line is referred to as simian line or “simian crease”. It is seen to be a merger between the “heart line” and the “head line.”[1],[2] It is considered that the prevalence of simian lines in general populations is usually 3%–5%. The simian line became well known considering its significance in Down's syndrome, but with advances in research, publications have linked simian lines with several syndromes and diseases.[1],[2] Suwon Crease (Line): this comprised a long heart line that crosses the entire palm appearing to join a head line at the radial edge and a second head line present. This line is considered by some writers as a “cousin” of the Sydney line. It is called Suwon Crease because the researchers who found it named it after their location in Suwon, Korea. It is said that the Korean researchers found it in 0.5% of 5196 hands. More commonly found in the left hand of males with 0.0% of females were found to have it in the Korean study.[1],[2] The Suwon line has the least diagnostic indication of all the creases. Sydney Line (crease) in 1967, Vrydagh-Laoureux mentioned that there is another line aside from the simian line. He called it an extended proximal palmar crease. This very line is known today as Sydney line. A line is said to be “Sydney line” when the proximal transverse crease extends beyond the midline axis of the fifth finger toward the ulna border of the palm. The Sydney line goes by its name because it was first discovered in Sydney.[1],[2] The presence of Sydney line is indicative of certain health conditions as in Alzheimer's dementia (gene is on chromosome 21), leukemia, and congenital rubella.[1],[2] There are a few observations on the distribution of simian and Sydney lines.[1],[2] It is stated that the Sydney line is more often found on the continent Australia and less often in Asia, while the simian crease is more often found in Asia.[1],[2] It is noted that there is a little difference in occurrence in sexes, the Sydney line can be observed more frequently in the hands of women, whereas the simian crease is known to be found slightly more often in the hands of men.[1],[2] It was reported in a study on Sydney line that the Sydney line is more often observed in the right, whereas the simian crease is known to be found more frequently in the left hand.[1],[2] Over the years, some researchers have done works on simian,[3],[4],[5],[6] Suwon,[7],[8] and Sydney creases [9],[10],[11],[12] in Caucasian populations.
Furuhata's Index
This is one of the indices or parameters used as a measure of comparison to determine the relationship between dermatoglyphic features. Rise in Furuhata's Index (FI) indicates the presence of a high percentage of whorls compared to the loops.[13]
To determine FI, the prints on the fingers are observed and identified as either arch, whorl, or loop which are summed up to have a total figure for each pattern before FI is calculated with the formula below:[13]
There is a paucity of literature on the palmar creases in acquired idiopathic blindness, particularly in Sub-Saharan Africa and Nigeria. This study is aimed at determining and comparing the prevalence of simian, Suwon, and Sydney creases in acquired idiopathic blindness.
| Materials And Methods | | |
Research design
A nonexperimental analytical design and palmar crease analysis model [14] were used. The finger and toeprint of the blind sampled from selected Special Schools and Centres for the Blind (Handicapped) in Nigeria (Oji River in Enugu State, Special Education School for the Blind in Afara-Ukwu, Umuahia in Abia State and Centre for Special Education, Creek Road, Borokiri, Port Harcourt) irrespective of ethnicity and age. The selection and collection of required parameters relied on informed consent of volunteers. This was done by reading them a copy of the informed consent letter. The nonblind participants were recruited from the same locality with the blind participants and had no known form of disease or disability using convenience purposive sampling. They freely gave their consent for the study by signing the informed consent form. A total number of 72 (36 blind and 36 nonblind) participants were recruited for the study that comprised 22 blind male and 14 blind female participants and 18 male and 18 female nonblind participants.
The sampling technique used was convenience purposive sampling.
Ethical clearance
Ethical clearance was sort from the Ethics Committee of the University of Port Harcourt.
Data collection
Hands were cleaned from dirt before taking prints, and a little pressure was put to press the palm on the scanner for adequate contact between the fingers and the scanner to have a clear image of the print and the prints were taken twice. The palm prints and toeprints were obtained using print scanner (Hp G3110 Photo Scanner). The prints were observed and analyzed using palmar crease analysis model [14] to see if there was simian, Suwon, or Sydney crease present in the palm. The toeprints were classified into arch, whorl, or loop patterns and counted.
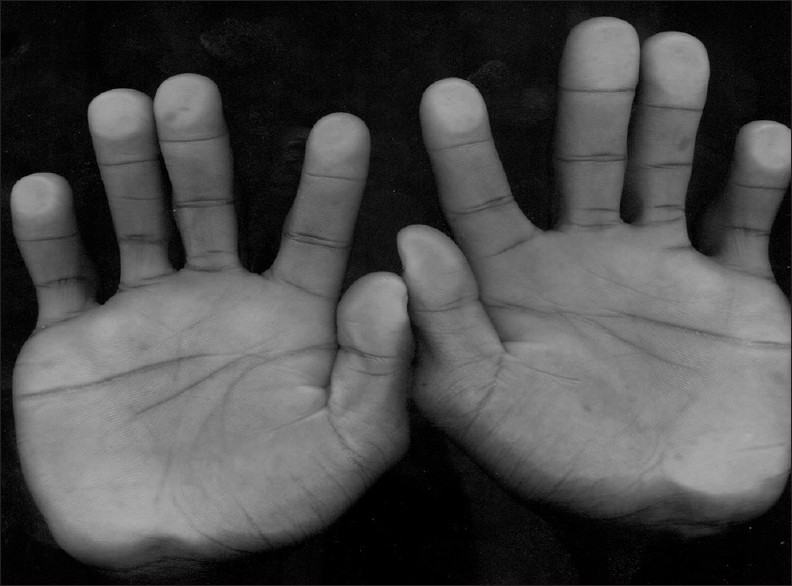
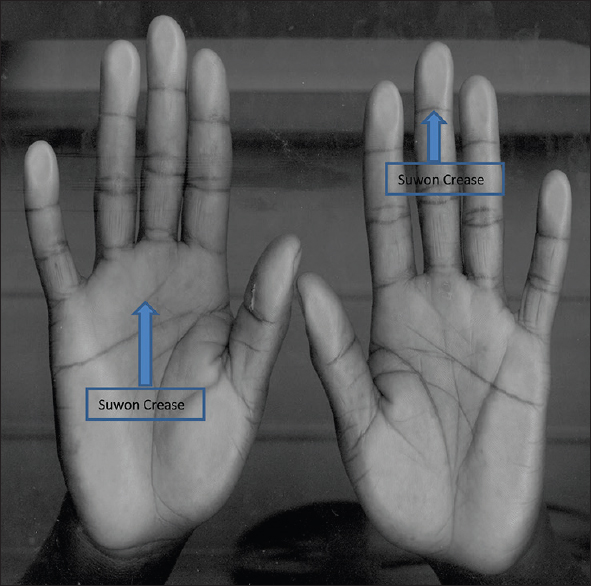
[Figure 1] shows the sydney crease on the palm. [Figure 2] shows the Suwon crease on the palm.
Data analysis
Data analysis was done using (IBM) Statistical Package for the Social Sciences version 22, and z-test of proportionality used to compare the prevalence of the creases using the distribution of the creases.
| Results | | |
The results of this study are as presented in the tables below. [Table 1] shows the prevalence of palmar creases in blind and nonblind male and female participants showed that the blind participants had 0% prevalence of simian crease, 3.8% prevalence of Suwon, and 0.6% prevalence of Sydney crease, whereas the nonblind participants have 0% prevalence of the creases. In the female blind participants, there was 0% prevalence of simian crease, 1.2% prevalence of Suwon, and 0.6% prevalence of Sydney crease, whereas the nonblind participants have 0% prevalence of the creases. The total prevalence of palmar creases of the blind and nonblind participants was shown, and the simian crease had 0.0% prevalence in the blind and in the nonblind participants. Suwon crease had 2.7% prevalence in the blind and 1.5% in the nonblind participants. Sydney crease had 0.6% prevalence in the blind, but 0% prevalence in the nonblind participants.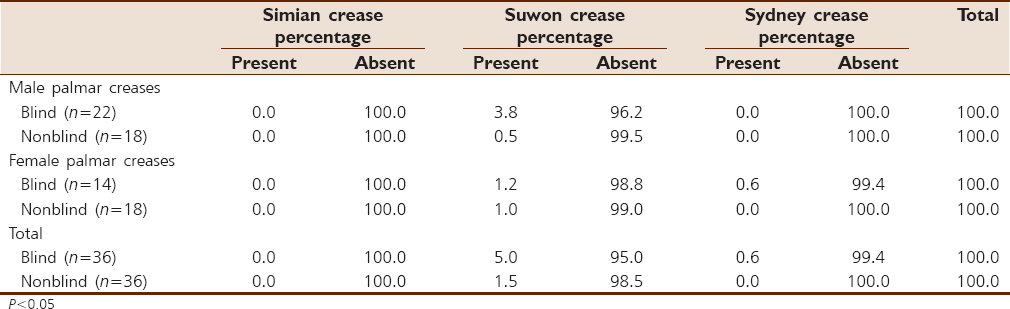 | Table 1: The prevalence of palmar creases (simian, Suwon, and Sydney) in both blind and nonblind participants
Click here to view |
[Table 2] shows FI for the blind males was 63.55 and nonblind males had 32.88, whereas the blind females had 75.73 and the nonblind females had 34.18. | Table 2: Furuhata's Index of the palm in the blind and nonblind participants
Click here to view |
| Discussion | | |
The prevalence of palmar creases in blind and nonblind male and female participants showed that there was the prevalence of Suwon crease in the blind males which was higher for the blind males than the nonblind males and also higher for the blind males than in the females. The prevalence of Sydney creases in the blind females but zero prevalence in the nonblind females. In the total prevalence of palmar creases of the blind and nonblind participants shown, the Suwon crease was the most prevalent palmar crease in the blind and nonblind followed by the Sydney crease in the blind participants. The blind participants had a higher prevalence of Suwon crease than the nonblind participants, It was observed that the blind subjects had a higher prevalence of Suwon crease which was not the same with the non-blind subjects, the Sydney crease had very little prevalence in the blind and zero prevalence in the non-blind subjects. Sentence reviewed, this difference could be attributed to a genetic interplay in the blind encouraging a higher prevalence. Comparing the prevalence of simian crease in this study with that of Oyinbo and Fawehinmi showed that the total prevalence obtained in their study was high, whereas in this present study, the prevalence of simian crease was zero. The prevalence of Sydney crease in their study was lesser than the prevalence obtained in this very study.
In FI, the females had higher values than the males consistently for the blind and nonblind participants, hence, indicating sexual dimorphism. This difference between the males and females was attributed to hormonal difference. This means that there was relatively higher frequency of whorls in the females than the males. In addition, on the average, FI was higher in the blind than in the nonblind participants which again points to the fact that there were more whorls present in blind than the nonblind which is attributed to genetic interplay in the blind participants.
| Conclusion | | |
The study has shown that there is no significant difference in the prevalence of Suwon and Sydney crease (P > 0.05), whereas there is a significant difference in the simian crease between the blind and nonblind compared. This study has provided information on the prevalence of palmar creases in people with idiopathic blindness and the nonblind people in Nigeria and by extension the Sub-Saharan Africa.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Oyinbo CA, Fawehinmi HB. Prevalence of simian and Sydney creases in the Ijaws of South-South Nigeria. Internet J Biol Anthropol 2009;3(2).  |
| 2. | Sharma DK, Sharma V. Prevalence of simian, Sydney and Suwon crease and their association with each other, body sides, handedness, gender and anomalies/diseases/syndromes in a population of Central India. Int J Morphol 2011;29:1069-75. |
| 3. | Chen YF, Zhang H, Shen CF, Lai CH. A dermatoglyphic study of the Amis aboriginal population of Taiwan. Sci China C Life Sci 2008;51:80-5. |
| 4. | Chen YF, Zhang H, Lai CH, Lu Z, Wang Z. A dermatoglyphic study of the Kavalan aboriginal population of Taiwan. Sci China C Life Sci 2007;50:135-9. |
| 5. | Iqbal S, Premalatha S, Zahra A. Dermatoglyphics in vitiligo. Int J Dermatol 1985;24:510-3. |
| 6. | Rajangam S, Janakiram S, Thomas IM. Dermatoglyphics in Down's syndrome. J Indian Med Assoc 1995;93:10-3. |
| 7. | Ciovîrnache M, Ioanitiu D, Ionescu B, Dumitrache C, Milea E, Dumitrache M. Dermatoglyphics in the virilizing polycystic ovary syndrome. Endocrinologie 198;24:87-96. |
| 8. | Oladipo GS, Okoh PD, Oghenemavwe LE, Yorkum LK. Dermatoglyphic patterns of autistic children in Nigeria. J Biol Agric Healthc 2013;3:80-3. |
| 9. | Borbolla L, Guerra D, Bacallao J. Dermatoglyphics in Cuban mongols. Acta Paediatr Acad Sci Hung 1980;21:107-21. |
| 10. | Balgir RS, Murthy RS, Wig NN. Genetic loadings in schizophrenia: a dermatoglyphic study. Isr J Med Sci 1993;29:265-8. |
| 11. | Bosco JI, Rajangam S, Shankar J, Thomas IM. Dermatoglyphics in 46, XY females. J Indian Med Assoc 2001;99:418-20. |
| 12. | Bartsocas CS, Panayotou T, Varonos S, Kritsikis S, Plato CC, Papadatos CJ. Digital and palmar dermatoglyphics in Greeks. Prog Clin Biol Res 1982;84:247-67. |
| 13. | Furuhata T. The difference of the index of finger prints according to race. Japan Med World 1927;(7):162-4. |
| 14. | Park JS, Shin DS, Jung W, Chung MS. Improved analysis of palm creases. Anat Cell Biol 2010;43:169-77. |
[Figure 1], [Figure 2]
[Table 1], [Table 2]
|








 Search Pubmed for
Search Pubmed for