|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2016 | Volume
: 4
| Issue : 2 | Page : 79-83 |
|
Comparative assessment on the prevalence of cusp of Carabelli among three different populations in India
Gayathri Ramesh1, Ramesh Nagarajappa2, Shitalkumar Sagari3, Gundareddy Nagendrareddy Suma4
1 Department of Oral and Maxillofacial Pathology, Rama Dental College Hospital and Research Centre, Kanpur, Uttar Pradesh, India
2 Department of Preventive and Public Health Dentistry, Institute of Dental Sciences, Bhuvaneshwar, Odisha, India
3 Department of Oral and Maxillofacial Pathology, Yogita Dental College and Hospital, Ratnagiri, Maharashtra, India
4 Department of Oral Medicine and Radiology, Faculty of Dental Sciences, SGT University, Gurgaon, Haryana, India
| Date of Web Publication | 18-Apr-2017 |
Correspondence Address:
Gayathri Ramesh
Department of Oral and Maxillofacial Pathology, Rama Dental College Hospital and Research Centre, Kanpur - - 208 024, Uttar Pradesh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2315-7992.204688

Background: The characteristics of a tooth can differ among races and species and can constantly alter due to natural selection and the genetic changes. Therefore, the study of the morphological properties of the dental structures could aid in phylogenic and genetic studies including gathering information about intra- and inter-species variations. Objectives: To assess and compare the prevalence of cusp of Carabelli among three different Indian (Rajasthan, Gujarat, and Karnataka) populations. Materials and Methods: A total of 200 casts (50% each of males and females) were evaluated for the presence or absence of Carabelli trait among the study population according to the scale of Dahlberg's (1963) scale. Casts of participants having maxillary first permanent molars bilaterally without gross damage to morphology by caries, attrition, or any other trauma were included in the study. Chi-square test with a significance level of P< 0.05 was used for statistical analysis. Results: The overall prevalence of Carabelli cusps was 57% (61% in males and 53% in females). The various groups showed a prevalence of 58.7%, 50%, and 61.7% in Rajasthan, Gujarat, and Karnataka population, respectively. The differences in the observations between groups and also gender were statistically insignificant (P > 0.05). The small vertical ridge and groove form were observed most commonly (31%), and small pit with minor grooves diverging from a depression form was the least prevalent (1.5%). Conclusions: The findings on the maxillary first permanent molar demonstrate that there was no significant difference in the prevalence of Carabelli cusps among the study populations.
Keywords: Carabelli's trait, India, prevalence
How to cite this article:
Ramesh G, Nagarajappa R, Sagari S, Suma GN. Comparative assessment on the prevalence of cusp of Carabelli among three different populations in India. Ann Bioanthropol 2016;4:79-83 |
How to cite this URL:
Ramesh G, Nagarajappa R, Sagari S, Suma GN. Comparative assessment on the prevalence of cusp of Carabelli among three different populations in India. Ann Bioanthropol [serial online] 2016 [cited 2017 Apr 29];4:79-83. Available from: http://www.bioanthrojournal.org/text.asp?2016/4/2/79/204688 |
| Introduction | |  |
All human populations have some degree of dental morphological variations.[1] The study of such characteristics is important in anthropological research because it can provide information on the phylogenetic relationship between species and variations within a population.[2],[3] It is commonly accepted that dental characteristics, such as size, shape, presence, number of cusps, and the size of the dental arches, are genetically determined.[4],[5]
The cusp of Carabelli is first described by George Carabelli in 1842.[6] It is a dental morphologic trait nonfunctioning mini cusp or tubercle or groove or furrow that presents symmetrically on the mesiopalatal surface of maxillary first permanent molar crowns.[7],[8] Although it is said that this cusp is not clinically important, it has some importance in dental industries, forensic odontology, and anthropology. The orthodontic molar bands have no compensation for this cusp. As a result, the space between the band and the tooth is filled with food debris, and it results in early caries and periodontal diseases. Furthermore, the Carabelli groove is a sensitive area for dental caries. This needs to be kept in mind during pit and fissure sealing. Even the molar extraction forceps have no accommodation for this cusp and may therefore result in fracture of the molar teeth.[8]
Cusp of Carabelli is entirely absent in some individuals and present in others in a variety of forms. It is a heritable feature and has been proposed that homozygosity of a gene is responsible for a pronounced tubercle, whereas the heterozygote shows as slight grooves, pits, tubercles, or bulge. It is expressed in several degrees and different frequencies between different populations.[2] It is most common among Europeans and rarest in Caucasians.[4] These variations are more pronounced in the case of Asian populations which points toward complex population history and extent of migration.[9] As the characteristics of a tooth can differ among races and species and can constantly alter due to natural selection and the genetic changes, an attempt was made to assess and compare the prevalence of cusp of Carabelli among three different Indian (Rajasthan, Gujarat, and Karnataka) populations.
| Materials and Methods | | |
The study protocol had been approved by the Ethical Committee at Pacific Dental College and Hospital, Udaipur, Rajasthan. The prevalence of Carabelli traits was based on plaster casts of the permanent dentition of 200 subjects (100 males and 100 females), which had been obtained from a randomly selected sample of 20–30 years old. They represented three different populations such as Rajasthan, Gujarat, and Karnataka. Casts of subjects having maxillary first permanent molars bilaterally without gross damage to morphology by caries, attrition, or any other trauma were included in the study. Exclusion criteria from the investigation were (i) poor quality of the study cast, (ii) chipped or broken teeth, (iii) wear or attrition, (iv) gross caries, and (v) restorations.
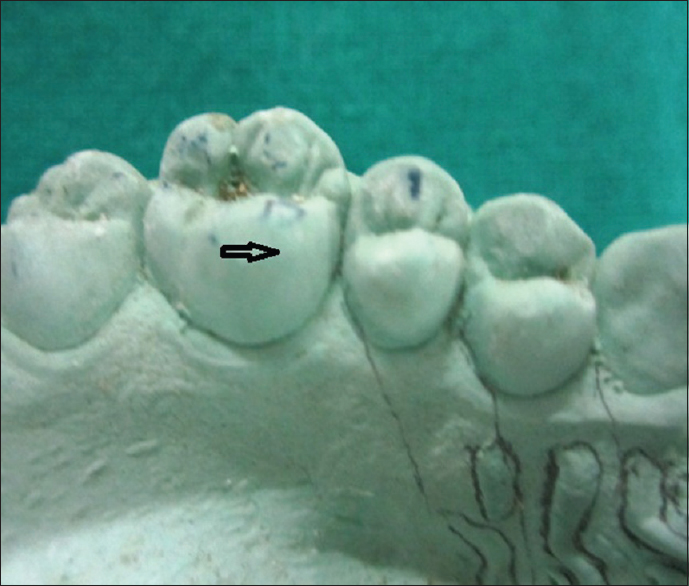
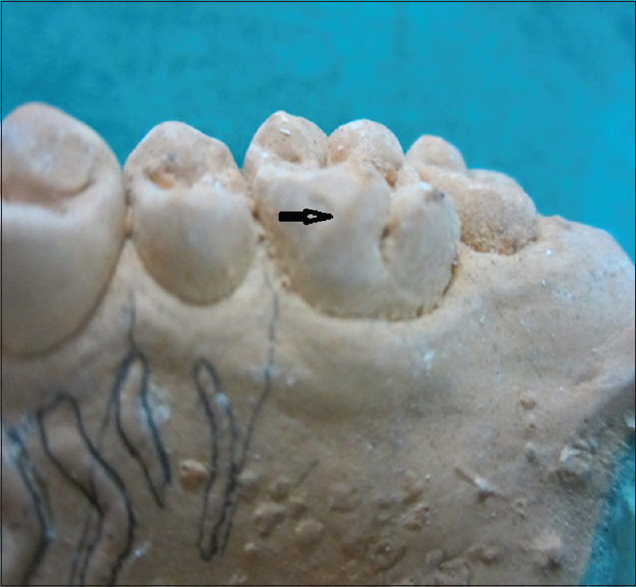
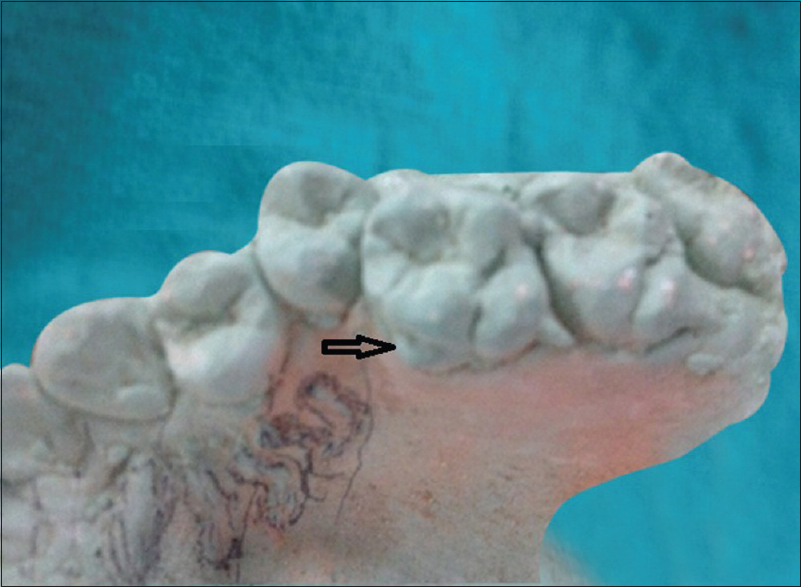
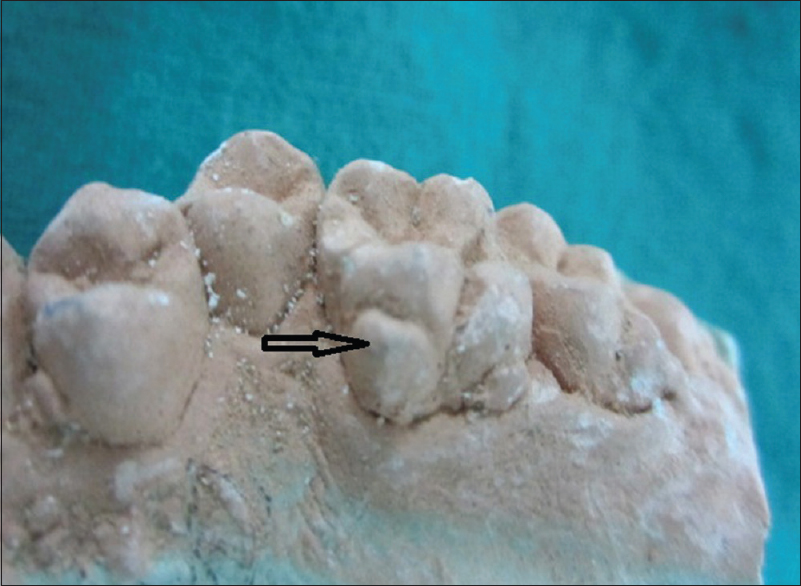
In the study cast examination, the maxillary first permanent molar on the casts [Figure 1],[Figure 2],[Figure 3],[Figure 4],[Figure 5],[Figure 6] was examined by one calibrated examiner (kappa = 0.90) using an illuminated magnifying glass (×2) to diagnose the presence or absence of a trait. The Dahlberg's scale (1963) criteria were employed to diagnose the Carabelli traits.[10]
- 0 - Smooth mesiobuccal crown surface
- 1 - Small vertical ridge and groove
- 2 - Small pit with minor grooves diverging from depression
- 3 - Double vertical ridges or slight and incomplete cusp outline
- 4 - Y-form (i.e., moderate grooves curving occlusally in opposite directions)
- 5 - Small tubercle
- 6 - Broad cusp outline with a moderate tubercle
- 7 - Large tubercle with a free apex.
Statistical analysis
To determine if there were any statistical differences between gender and population groups, the Chi-square test was used to test the quantity of proportions. The level of statistical significance was fixed at P< 0.05.
| Results | | |
In this study, a total of 200 casts were examined for the presence or absence of cusp of Carabelli. Of these 200 casts, 100 each were of males and females. The three population groups included were Rajasthan (eighty casts), Gujarat (sixty casts), and Karnataka (sixty casts) [Table 1]. The overall prevalence of Carabelli cusps in maxillary first permanent molar was 57% (61% in males and 53% in females). The small vertical ridge and groove form were observed most commonly (31%), and small pit with minor grooves diverging from a depression form was the least prevalent (1.5%) [Table 2].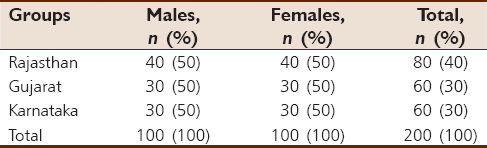 | Table 1: Distribution of the study population according to groups and gender
Click here to view |
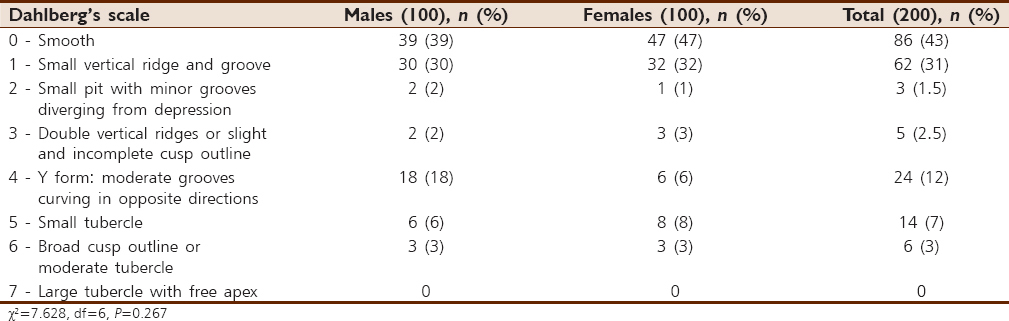 | Table 2: Distribution of the Dahlberg's scale scores according to gender
Click here to view |
The various groups showed a prevalence of 58.7%, 50%, and 61.7% in Rajasthan, Gujarat, and Karnataka population, respectively. An almost equal distribution was observed among males and females in both Rajasthan and Gujarat populations, but the Karnataka population showed a clear male predominance. Small vertical ridge and groove were most commonly observed followed up with Y form: Moderate grooves curving in opposite directions among all the populations. It was concluded that the prevalence of cusp of Carabelli is lowest in the population sample of Gujarat as compared to other population's samples. The differences in the observations between groups and also gender were statistically insignificant (P > 0.05) [Table 3].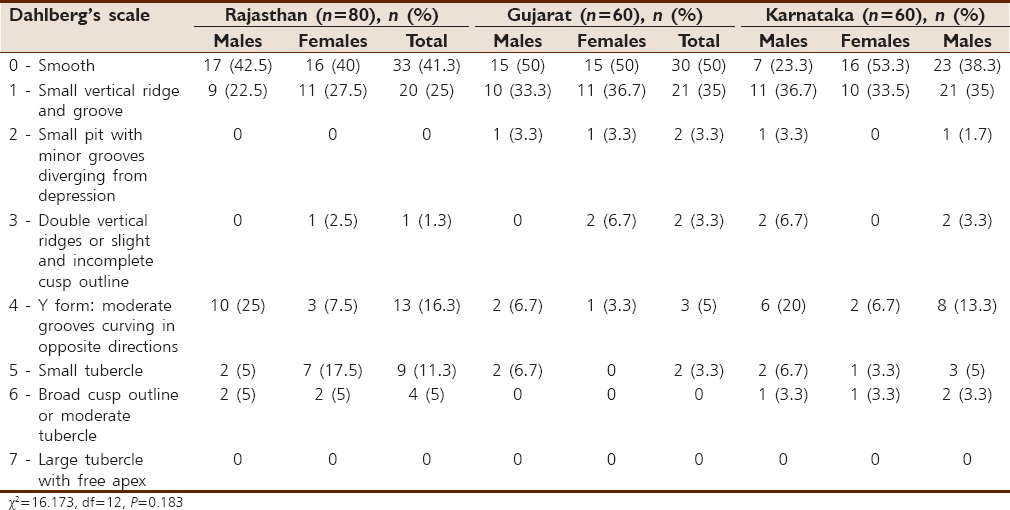 | Table 3: Distribution of the Dahlberg's scale scores among the different groups
Click here to view |
| Discussion | | |
Local populations in India are difficult to define because the population consists of many races of different origins. Therefore, much confusion prevails about the origin of any population. However, the most predominant populations in India which in a broad sense denotes common ethnic origin were studied. Therefore, the present study is confined to observations on Carabelli's trait in three different populations.
Carabelli's cusp itself has many synonyms. Kraus designated it an anomaly because it occurs in a variety of morphologic forms. It has been called Carabelli's cusp, tubercle, structure, or even tuberculum impar.[11] Nevertheless, because it denotes the presence of a particular characteristic, “trait” is the most appropriate term.[12]
The prevalence of cusp of Carabelli was 57% in this study. These findings were in agreement with the similar studies where the prevalence of cusp of Carabelli was reported to be 52.2%, 58.7%, 52.7%, and 65.3%, respectively [8,13-15] but deviated widely from the studies by Hassanali [16] who reported the prevalence of this cusp to be 26%–27% in Asian school children. Mosharraf in 2013 has reported a higher prevalence of 96.6% among Iranian adolescents.[17]
In this study, more males had cusp of Carabelli (61%) than females (53%). This was in agreement with the report by Kamatham and Nuvvula, wherein males showed a greater representation of positive trait (34.6%) than females (25.5%) among children of Nellore population, Andhra Pradesh, India.[18] But in contrast with the results of higher incidence among females (53.5%) than males (46.5%) as reported by Salako and Bello in 1998 among children of the Saudi Arabian population.[14] The reason for more males having cusp of Carabelli was reported to be the more complex nature of crowns in males than females. However, several researchers have revealed that there are reported no sexual preference in the overall prevalence of the trait.[17],[19],[20]
The most common form of this cusp observed in this study was small vertical ridge and groove form (31%), and small pit with minor grooves diverging from a depression form was the least prevalent (1.5%). Other studies reported a small tubercle predominantly.[21]
Carabelli's trait appears to be generally common among European populations, followed by African populations, and American Indians, with the lowest prevalence occurring in the other Mongoloid races.[20] However, the prevalences of 50.5% for Southern Chinese are comparable to the prevalence for our population groups 58.7%, 50%, and 61.7% in Rajasthan, Gujarat, and Karnataka populations, respectively.[20] The general trend is for this trait to be more common in Southern Chinese than other Mongoloid groups. When only the tubercle and cusp forms were considered, the pattern of geographic variation in Carabelli's trait is not particularly striking.[22]
On the whole, frequencies of occurrence of Carabelli trait were found between populations in the present study though it was insignificant. Some of the variation in the published data for different populations probably reflects the use of different diagnostic criteria by the investigators rather than a real difference.
| Conclusions | | |
This study showed that more than 50% of the study populations expressed Carabelli's trait on their maxillary first permanent molars. However, the difference in their prevalence was not significant. When dental records are not available, dental traits can give clues and aid forensic identification of the victim.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Jerome CE, Hanlon RJ Jr. Dental anatomical anomalies in Asians and Pacific Islanders. J Calif Dent Assoc 2007;35:631-6.  |
| 2. | Palomino H, Chakraborty R, Rothhammer F. Dental morphology and population diversity. Hum Biol 1977;46:61-70. |
| 3. | Sharma JC. Dental morphology and odontometry of the Tibetan immigrants. Am J Phys Anthropol 1983;61:495-505. |
| 4. | Goose DH, Lee GT. The mode of inheritance of Carabelli's trait. Hum Biol 1971;43:64-9. |
| 5. | Stamfelj I, Stefancic M, Gaspersic D, Cvetko E. Carabelli's trait in contemporary Slovenes and inhabitants of a medieval settlement (Sredisce by the Drava River). Coll Antropol 2006;30:421-8. |
| 6. | Mellor JK, Ripa LW. Talon cusp: A clinically significant anomaly. Oral Surg Oral Med Oral Pathol 1970;29:225-8. |
| 7. | Reid C, van Reenen JF, Groeneveld HT. Tooth size and the Carabelli trait. Am J Phys Anthropol 1991;84:427-32. |
| 8. | Kannapan JG, Swaminathan S. A study on a dental morphological variation. Tubercle of Carabelli. Indian J Dent Res 2001;12:145-9. |
| 9. | Hanihara T. Morphological variation of major human populations based on nonmetric dental traits. Am J Phys Anthropol 2008;136:169-82. |
| 10. | Kieser JA, van der Merwe CA. Classificatory reliability of the Carabelli trait in man. Arch Oral Biol 1984;29:795-801. |
| 11. | Kraus BS. Carabelli's anomaly of the maxillary molar teeth; observations on Mexicans and Papago Indians and an interpretation of the inheritance. Am J Hum Genet 1951;3:348-55. |
| 12. | Joshi MR, Godiawala RN, Dutia A. Carabelli's trait in Hindu children from Gujarat. J Dent Res 1972;51:706-11. |
| 13. | Rusmah M. The cusp of Carabelli in Malaysians. Odontostomatol Trop 1992;15:13-5. |
| 14. | Salako NO, Bello LL. Prevalence of the Carabelli trait in Saudi Arabian children. Odontostomatol Trop 1998;21:11-4. |
| 15. | Mavrodisz K, Rózsa N, Budai M, Soós A, Pap I, Tarján I. Prevalence of accessory tooth cusps in a contemporary and ancestral Hungarian population. Eur J Orthod 2007;29:166-9. |
| 16. | Hassanali J. Incidence of Carabelli's trait in Kenyan Africans and Asians. Am J Phys Anthropol 1982;59:317-9. |
| 17. | Mosharraf R. Prevalence of the Carabelli trait in Iranian adolescents. SRM J Res Dent Sci 2013;4:12-5. [Full text] |
| 18. | Kamatham R, Nuvvula S. Expression of Carabelli trait in children from Southern India – A cross sectional study. J Forensic Dent Sci 2014;6:51-7. [ PUBMED] [Full text] |
| 19. | Dissanayake U, Chandrasekera MS, Wikramanayake ER. The prevalence and mode of inheritance of Carabelli trait in the Sinhalese. Ceylon J Med Sci 2004;47:7-15. |
| 20. | King NM, Tsai JS, Wong HM. Morphological and numerical characteristics of the Southern Chinese dentitions. Part II: Traits in the permanent dentition. Open Anthropol J 2010;3:71-84. |
| 21. | Khan DB, Khan MA, Khattak M. Prevalence of cusp of Carabelli in permanent teeth in a group from Khyber Pakhtunkhwa, Pakistan. Pak Oral Dent J 2011;31:409-11. |
| 22. | Scott GR, Turner CG. The Anthropology of Modern Human Teeth: Dental Morphology and Its Variations. Cambridge: Cambridge University Press; 1997. p. 197-201. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6]
[Table 1], [Table 2], [Table 3]
|










 Search Pubmed for
Search Pubmed for