|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2017 | Volume
: 5
| Issue : 1 | Page : 18-21 |
|
Determination of the palmar ridge counts and angles in acquired idiopathic blindness in some selected schools for the blind in Nigeria
JN Paul, EA Osunwoke, CW Paul
Department of Human Anatomy, Faculty of Basic Medical Sciences, College of Health Sciences, University of Port Harcourt, Port Harcourt, Nigeria
| Date of Web Publication | 11-Jul-2017 |
Correspondence Address:
E A Osunwoke
Department of Human Anatomy, Faculty of Basic Medical Sciences, College of Health Sciences, University of Port Harcourt, Port Harcourt
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2315-7992.210249

Background: Ridges are delicately sculpted skin surface and their configural arrangements present on human fingers, toes, and soles. Aim: This study was aimed at determining the palmar ridge counts and palmar angles in acquired idiopathic blindness. Materials and Methods: The study had 72 subjects comprising 36 blind (14 females and 22 males) and 36 nonblind (18 females and 18 males). Palmar prints were obtained using print scanner (HP G3110 Photo Scanner). Results: The mean and standard deviation of the ridge counts for the total blind subjects: on the right hand, A–B was 26.02 ± 2.96, B–C was 27.04 ± 2.81, C–D was 33.16 ± 3.55; and on the left hand, A–B was 26.51 ± 2.38, B–C was 26.99 ± 2.89, and C–D was 33.20 ± 3.44. Considering the total ridge counts for the nonblind subjects on the right hand: A-B was 35.53 ± 1.99, B-C was 22.83 ± 1.87, and C-D was 41.20 ± 2.75; and on the left hand: A-B was 32.72 ± 2.54, B-C was 22.89 ± 2.24, and C-D was 41.30 ± 2.57. The palmar angles had the following values for the blind: on the right hand, ATD angle was 38.69° ± 3.65°, DAT angle was 60.11° ± 4.45°, and TDA angle was 81.19° ± 4.06°, while on the left hand: ATD angle was 38.47° ± 4.14°, DAT angle was 60.28° ± 4.49°, and TDA angle was 81.19° ± 4.50°. Conclusion: This study provides baseline information for researchers who will find it relevant in the course of their research with respect to palmar ridge counts and angles. Keywords: Angles, idiopathic blindness, Nigeria, ridge counts
How to cite this article:
Paul J N, Osunwoke E A, Paul C W. Determination of the palmar ridge counts and angles in acquired idiopathic blindness in some selected schools for the blind in Nigeria. Ann Bioanthropol 2017;5:18-21 |
How to cite this URL:
Paul J N, Osunwoke E A, Paul C W. Determination of the palmar ridge counts and angles in acquired idiopathic blindness in some selected schools for the blind in Nigeria. Ann Bioanthropol [serial online] 2017 [cited 2018 Jul 8];5:18-21. Available from: http://www.bioanthrojournal.org/text.asp?2017/5/1/18/210249 |
| Introduction | |  |
Ridges are delicately sculpted skin surface and their configural arrangements present on human fingers, toes, and soles.[1] Dermal ridges originate from fetal volar pads made up of mesenchymal tissue beginning at the 6th–7th week of intrauterine life. The size and position of the volar pads are pivotal in the presentation of the ridge patterns.[1] It further suggests that small pads produce arches and larger pads produce loops or whorls. A shift of the volar pad laterally induces asymmetry in the pattern of the ridges. Ridges become visible at about 3 months and are completed by the 6th month of prenatal development.[1] Dermatoglyphic patterns result from convolutions of layers of cells of the epidermis of the skin. The pore of the sweat glands are located at the peak of the ridges.[1] Ridges are formed during embryonic stage of the growth and remain unchanged after birth. However, extensive physical labor can wear them down and scars can distort the pattern.[1]
Ridge counts [2],[3] and palmar angles [4] have been done in a whole lot of studies as in polydactyl,[5] constitutional exogenous adiposity,[4] schizophrenia,[6] even among nations such as in Spanish populations,[7] Sardinians,[8] Northwest Indians,[9] Bulgarians,[10] Zimbabweans,[11] and Kenyans and Tanzanians.[12]
| Materials and Methods | | |
Research design
The finger and toe prints of the blind sampled from selected special schools and centers for the blind (handicapped) in Nigeria (Oji River in Enugu State, Special Education School for the Blind in Afara-Ukwu, Umuahia in Abia State, Centre for Special Education, Creek Road, Borokiri, Port Harcourt), irrespective of ethnicity and age. The selection and collection of required parameters relied on informed consent of volunteer subjects. This was performed by reading them a copy of the informed consent letter. The palm prints were obtained using a print scanner (HP G3110 Photo Scanner). A total of 72 (36 blind and 36 nonblind) participants were recruited for the study that comprised 22 blind male and 14 blind female participants and 18 male and 18 female nonblind participants. [Figure 1] shows the structure of ridge patterns in the finger.[13]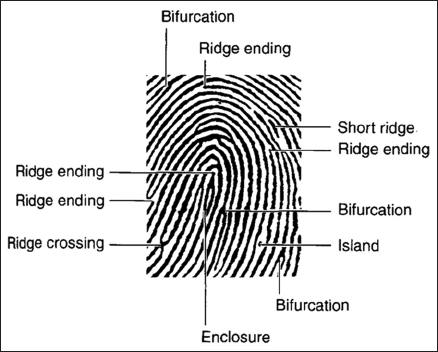 | Figure 1: The structure of minutiae showing ridges (www.newscientist.com, 2015)
Click here to view |
The sampling technique used was purposeful sampling, and ethical clearance was obtained from the Ethics Committee of the University of Port Harcourt.
Data collection
AutoCAD software (AutoCAD 360 version 1.3 by Autodesk, Incorporated. 2011. San Rafael, California: United States of America) was used to make a straight line from the core of one triradius to the next triradius and the number of complete ridges that cut across the straight line was counted for A–B, B–C, and C–D ridge counts. For palmar angles, the three triradii were located and identified from the base of the index finger as “a,” base of the little finger as “d,” and base of the palm as “t” after which, a straight line was taken “a” to “d” down to “t” and back to “a” forming a triangle. To determine each angle, the angular dimension tool on the AutoCAD was used. The angular tool was placed on both lines connecting the angle and clicked which indicated the angular dimension for each of the angles (ATD, TDA, and DAT). At the end, the data gotten were recorded for computation.
Data analysis
Data analysis was carried out using IBM SPSS Statistics for Windows, Version 22.0. IBM Corp. 2013 Armonk, New York: United States.
| Results | | |
The results of this study are presented in [Table 1] and [Table 2].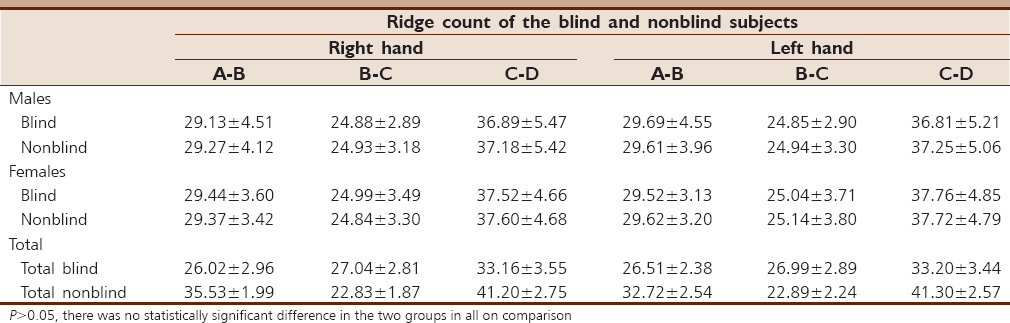 | Table 1: The mean and standard deviation of the ridge counts in both blind and nonblind males and females
Click here to view |
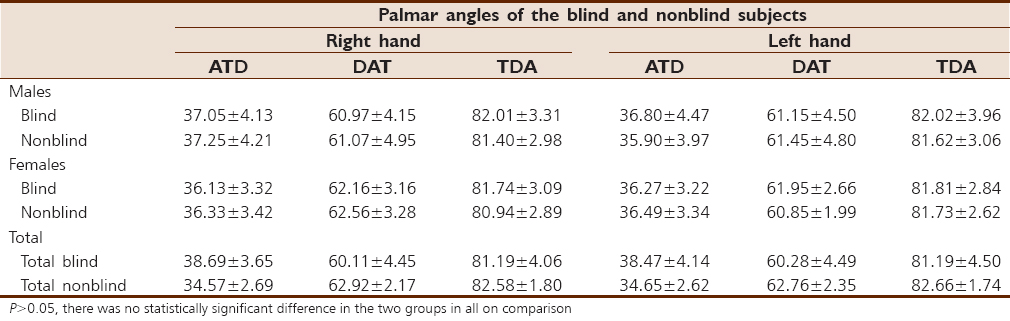 | Table 2: The mean and standard deviation of the palmar angles in both blind and nonblind males and females
Click here to view |
In [Table 1], the mean and standard deviation of the ridge counts for the total blind subjects: on the right hand, A–B was 26.02 ± 2.96, B–C was 27.04 ± 2.81, C–D was 33.16 ± 3.55; and on the left hand, A–B was 26.51 ± 2.38, B–C was 26.99 ± 2.89, and C–D was 33.20 ± 3.44. Considering the total ridge counts for the nonblind subjects on the right hand: A-B was 35.53 ± 1.99, B-C was 22.83 ± 1.87, and C-D was 41.20 ± 2.75; and on the left hand: A-B was 32.72 ± 2.54, B-C was 22.89 ± 2.24, and C-D was 41.30 ± 2.57. In the blind male subjects, on the right hand: A–B was 29.13 ± 4.51, B–C was 24.88 ± 2.89, and C–D was 36.89 ± 5.47; and on the left hand: A–B was 29.69 ± 4.55, B–C was 24.85 ± 2.90, and C–D was 36.81 ± 5.21. Considering the nonblind male subjects, on the right hand: A–B was 29.27 ± 4.12, B–C was 24.93 ± 3.18, and C–D was 37.18 ± 5.42; and on the left hand: A–B was 29.61 ± 3.96, B–C was 24.94 ± 3.30, and C–D was 37.25 ± 5.06. In the blind female subjects, on the right hand: A–B was 29.44 ± 3.60, B–C was 24.99 ± 3.49, and C–D was 37.52 ± 4.66; and on the left hand: A–B was 29.52 ± 3.13, B–C was 25.04 ± 3.71, and C–D was 37.76 ± 4.85. Considering the nonblind female subjects, on the right hand: A–B was 29.37 ± 3.42, B–C was 24.84 ± 3.30, and C–D was 37.60 ± 4.68; and on the left hand: A–B was 29.62 ± 3.20, B–C was 25.14 ± 3.80, and C–D was 37.72 ± 4.79.
In the male subjects, the TDA was consistently high, followed by the DAT and finally the ATD. For the blind subjects: on the right hand, the ATD angle was 37.05 ± 4.13, DAT angle was 60.97 ± 4.15, and TDA angle was 82.01 ± 3.31; on the left hand, the ATD angle was 36.80 ± 4.47, DAT angle was 61.15 ± 4.50, and TDA angle was 82.02 ± 3.96. For the nonblind subjects: on the right hand, the ATD angle 37.25 ± 4.21, DAT was 61.07 ± 4.95, and TDA was 81.40 ± 2.98, whereas on the left hand, ATD angle was 35.90 ± 3.97, DAT angle was 61.45 ± 4.80, and TDA was 81.62 ± 3.06.
In the female subjects, the TDA was consistently high, followed by the DAT and finally the ATD. For the blind female subjects: on the right hand, the ATD angle was 36.13 ± 3.32, DAT angle was 62.16 ± 3.16, and TDA angle was 81.74 ± 3.09; on the left hand, the ATD angle was 36.27 ± 3.22, DAT angle was 61.95 ± 2.66, and TDA angle was 81.81 ± 2.84. For the nonblind female subjects: on the right hand, the ATD angle was 36.33 ± 3.42, DAT was 62.56 ± 3.28, and TDA was 80.94 ± 2.89; whereas on the left hand, ATD angle was 36.49 ± 3.34, DAT angle was 60.85 ± 1.99, and TDA was 81.73 ± 2.62 [Table 2].
In [Table 2], the mean and standard deviation of the palmar angles in the total blind and nonblind subjects was shown as follows: For the blind: on the right hand, the ATD angle was 38.69 ± 3.65, DAT angle was 60.11 ± 4.45, and TDA angle was 81.19 ± 4.06, while on the left hand, ATD angle was 38.47 ± 4.14, DAT angle was 60.28 ± 4.49, and TDA angle was 81.19 ± 4.50. For the nonblind subjects: on the right hand, the ATD angle was 34.57 ± 2.69, DAT angle was 62.92 ± 2.17, and TDA angle was 82.58 ± 1.80; whereas on the left hand, the ATD angle was 34.65 ± 2.62, DAT angle was 62.76 ± 2.35, and the TDA angle was 82.66 ± 1.74.
| Discussion | | |
In the male subjects, it was noted that the C–D ridge count was consistently high, followed by the A–B ridge count and then B–C ridge count. For the blind males, A–B ridge count was lesser on the right hand than the left hand, and B–C ridge count and C–D ridge count were more on the right than the left hand. In the nonblind male subjects, the A–B, B–C, and C–D ridge counts were all lesser on the right hand than the left hand. Between the blind and nonblind male subjects, on the right hand, the A–B and B–C ridge counts were higher in the nonblind than the blind whereas the C–D ridge count was higher in the blind and nonblind subjects; and on the left hand, the A–B ridge count was higher in the blind than the nonblind, B–C ridge count was higher in the nonblind than the blind, whereas the C–D ridge count was higher in the blind than the nonblind. The difference between the ridge counts in the blind and nonblind subjects was attributed to genetic interplay in the blind subjects.
In the female subjects, the C–D ridge count was consistently high, followed by the A–B ridge count and then the B–C ridge count. In the blind females, the A–B, B–C, and C–D ridge counts were lesser on the right hand than the left hand. Again, in the nonblind females, the A–B, B–C, and C–D ridge counts were lesser on the right hand than the left hand as it was for the blind subjects. Between the blind and nonblind subjects: on the right hand, the A–B and B–C ridge counts were higher in the blind than the nonblind subjects, but the C–D ridge count was higher in the nonblind subjects than the blind subjects. Between the blind and nonblind subjects: on the left hand, A–B and B–C ridge counts were higher in the nonblind than the blind subjects, but the C–D ridge count was higher in the blind subjects than the nonblind subjects. It suggests that there was a genetic input which accounts for the difference between the ridge counts in the blind and nonblind subjects.
However, in the male subjects, the TDA was consistently high, followed by the DAT and finally the ATD. For the blind subjects, ATD and DAT angles were higher on the right than the left hand whereas TDA was lesser on the right than the left hand. For the nonblind subjects, the ATD and TDA angles were lesser on the right hand than the left hand whereas the DAT angle was higher on the right than left hand. Between the blind and nonblind subjects: on the right hand, the ATD angle was higher in the nonblind than the blind while the DAT and TDA angles were lesser in the nonblind than the blind subjects; whereas on the left hand, ATD, DAT and TDA angles were higher in the nonblind than the blind subjects. The difference between the angles in the blind and nonblind subjects was attributed to genetic interplay in the blind subjects.
In addition, in the female subjects, the TDA was consistently high, followed by the DAT and finally the ATD. For the blind and nonblind subjects, the ATD and TDA angles were lesser on the right than the left hand while DAT angle was higher on the right than the left hand. Between the blind and nonblind subjects: on the right hand, the ATD and DAT were higher in the nonblind than the blind but TDA was lesser in the nonblind than blind subjects whereas on the left hand, ATD angle was higher on the nonblind than the blind but DAT and TDA angles were lesser in the nonblind than blind subjects. There were indications of genetic input as in the males.
| Conclusion | | |
This study provides anthropometric data for researchers and forensic experts and in medical diagnosis relevant to dermatologists.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Mohd Bhat G, Arif Mukhdoomi M, Bahir Ahmed S, Mohd Saleem I. Dermatoglyphics: In health and disease – A review. Int J Res Med Sci 2014;2:31-7.  |
| 2. | 2. Anibor E, Eboh DE, Okumagba MT, Etetafia MO. Palmar and digital dermatoglyphic patterns of the Ijaws in Delta State of Nigeria. Arch Appl Sci Res 2011;3:301-6. |
| 3. | Anibor E, Igbigbi PS, Avwioro OG, Okpor A. Palmar and digital dermatoglyphic patterns in the Ndokwas of Delta State, Nigeria. Afr J Med Med Sci 2011;40:181-5. |
| 4. | Kaladze NN, Chebanova NA, Doroshenko LK. Dermatoglyphics in children with constitutional exogenous obesity. Probl Endokrinol (Mosk) 1992;38:23-4. |
| 5. | Oladipo GS, Okoh PD, Agi C, Dike EU, Orluwene CG. A comparative study of dermatoglyphic patterns of polydactyly patients and normal Nigerian individuals. Int J Pharm Appl 2013;4:38-42. |
| 6. | Fañanás L, Moral P, Bertranpetit J. Quantitative dermatoglyphics in schizophrenia: study of family history subgroups. Hum Biol 1990;62:421-7. |
| 7. | Martín J, Portabales D. Quantitative finger dermatoglyphics in a Spanish population (Tierra de Campos). Anthropol Anz 1986;44:227-38. |
| 8. | Sanna E, Vallascas E, Usai E, Floris G. Quantitative digital and palmar dermatoglyphics among Sardinian linguistic groups. Anthropol Anz 2007;65:365-82. |
| 9. | Reddy BM, Chopra VP, Karmakar B, Malhotra KC, Mueller H. Quantitative dermatoglyphics and population structure in Northwest India. Am J Hum Biol 2000;12:315-26. |
| 10. | Tornjova-Randelova S, Borissova P, Paskova-Topalova D. Quantitative characterization of finger and palm dermatoglyphics in Bulgarians. Anthropol Anz 2008;66:295-315. |
| 11. | Igbigbi PS, Msamati BC. Palmar and digital dermatoglyphics of indigenous black Zimbabweans. Med Sci Monit 2002;8:CR757-61. |
| 12. | Igbigbi PS, Msamati BC. Palmar and digital dermatoglyphic traits of Kenyan and Tanzanian subjects. West Afr J Med 2005;24:26-30. |
| 13. | |
[Figure 1]
[Table 1], [Table 2]
|








 Search Pubmed for
Search Pubmed for