| |


 |
| Year : 2011 | Volume
: 5
| Issue : 3 | Page : 68-71 |
|
|
|
|
|
ORIGINAL ARTICLE Arthroscopic evaluation and treatment of biceps brachii long head tendon injuries: A survey of the MOON shoulder group
Timothy Miller, Grant Jones, Moon Shoulder Group
Department of Orthopaedics, The Ohio State University Medical Center, OSU Sports Medicine Center, Columbus, OH, USA
Correspondence Address:
Grant Jones
OSU Sports Medicine Center, 2050 Kenny Road, Suite 3100, Columbus, OH 43221 3502
USA
 Source of Support: None, Conflict of Interest: None  | 4 |
DOI: 10.4103/0973-6042.86236

|
|
|
|
| Date of Web Publication | 17-Oct-2011 |
 Abstract Abstract | | |
Context: Injuries to the biceps brachii long head tendon commonly occur in conjunction with tears in the rotator cuff and glenoid labrum. Consensus on treatment of varying levels of severity is undetermined.
Settings and Design: We surveyed members of the Multicenter Orthopedic Outcomes Network (MOON) Shoulder Group, to determine a consensus on arthroscopic grading and treatment.
Aims: We hypothesized that the Lafosse classification system would show a high level of inter- and intraobserver agreement regarding grading/treatment.
Materials and Methods: Arthroscopic videos of 30 patients determined to have biceps brachii long head tendon injuries were viewed by 13 surgeons. The surgeons graded the severity of the injury macrostructure based on the Lafosse classification system and chose from a list of treatment options. Four months later the same surgeons viewed the same videos and repeated the survey.
Statistical Analysis Used: Analysis with weighted and non-weighted Kappa values was performed to determine intra- and interobserver reliability for severity grading and to determine the preferred treatments for each level of severity.
Results: Intraobserver reliability testing for the Lafosse system showed substantial agreement after two rounds (81.28%, K=0.7006). Interobserver testing demonstrated substantial agreement for Grade 0 (K=0.7152), fair agreement for Grade 1 (K=0.3803), and moderate agreement for Grade 2 (K=0.5156). Combined responses recommended no surgical treatment for 95.4% of the lesions classified as grade 0 (62/65). No surgical treatment was recommended for Grade 1 lesions in 24.1% of the cases (35/145), debridement in 38.6% (56/145), and tenotomy or tenodesis in 37.2% (54/145). Evaluators preferred tenotomy or tenodesis for 98.3% of the Grade 2 lesions (177/180).
Conclusions: Analysis of the Lafosse system indicated substantial intraobserver reliability for all grades. As Grades 1 and 2 showed only fair and moderate agreement, a need for a reliable grading system still exists. Grade 2 lesions should be treated with tenotomy or tenodesis. A preferred treatment for Grade 1 lesions could not be determined given the high variability of responses. Higher-powered surveys may help determine the ideal treatment of Grade 1 injuries.
Keywords: Arthroscopic grading systems, biceps brachii, intraobserver reliability
How to cite this article:
Miller T, Jones G, Moon Shoulder Group. Arthroscopic evaluation and treatment of biceps brachii long head tendon injuries: A survey of the MOON shoulder group. Int J Shoulder Surg 2011;5:68-71 |
| Introduction | |  |
The biceps brachii long head tendon is a common source of pain in patients with shoulder pathology. Injuries to the tendon commonly occur in conjunction with tears of the rotator cuff and the glenoid labrum. To date, no clearly defined treatment protocol for injuries to this tendon has been established. As a consensus on the treatment of the varying levels of severity has yet to be determined, treatment preferences for biceps brachii long head injuries vary from surgeon to surgeon.
A validated system for classifying these injuries is necessary for standardizing their treatment. Of late, the Lafosse classification system [1] [Table 1] has been proposed and employed for evaluation and grading of these injuries. [2],[3],[4] However, currently neither the Lafosse classification system nor any other grading system of the biceps brachii long head tendon injuries has undergone testing for inter-and intraobserver reliability between fellowship-trained shoulder surgeons.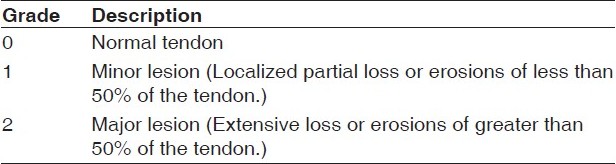 | Table 1: The Lafosse classification system (L. Lafosse et al., Arthroscopy, January 2007)
Click here to view |
The purpose of this study is to survey members of the MOON Shoulder Group and determine a consensus on the arthroscopic grading and ideal treatment for biceps tendon injuries. The authors employed two hypotheses for this study: (1) The Lafosse classification system would show a high level of inter- and intraobserver agreement for grading injuries to the biceps brachii long head tendon; and (2) There would be a high level of agreement between the shoulder surgeons for treatment of biceps tendon injuries of varying severity.
| Materials and Methods | | |
After approval for exemption from the Institutional Review Board (IRB) proceedings at our institution, arthroscopic videos were collected prospectively for 30 patients who underwent shoulder arthroscopy procedures. All surgeries were performed by the same surgeon at one institution. All patients had previously presented to the surgeon's clinic with shoulder symptoms indicative of biceps tendon injuries. During all the procedures, a video recording was done when the biceps tendon was probed and examined.
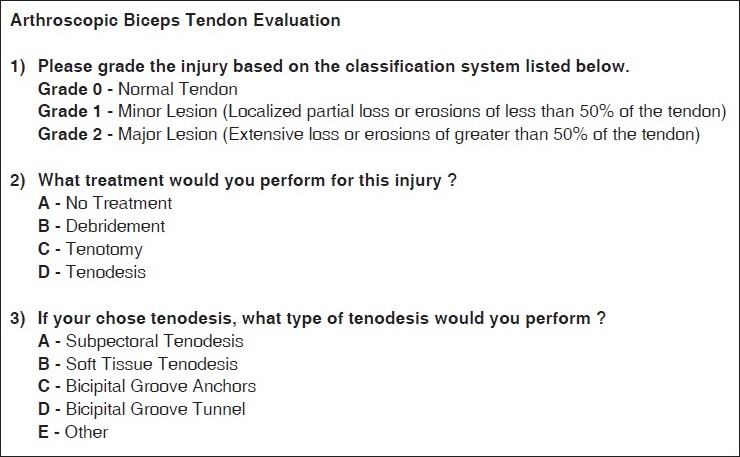
Arthroscopic videos [Figure 1],[Figure 2],[Figure 3] were viewed by 13 members of the Multicenter Orthopedic Outcomes Network (MOON) Shoulder Group. All evaluators were fellowship-trained shoulder surgeons, with varying levels of experience. Each member of the group was asked to grade the severity of the injury macrostructure of the tendon based on the static portion of the classification system of Lafosse et al. [1] They were then asked to choose from the list of treatment options for the injury [Figure 4]. Treatment options listed on this survey included: No treatment, debridement, tenotomy, and tenodesis.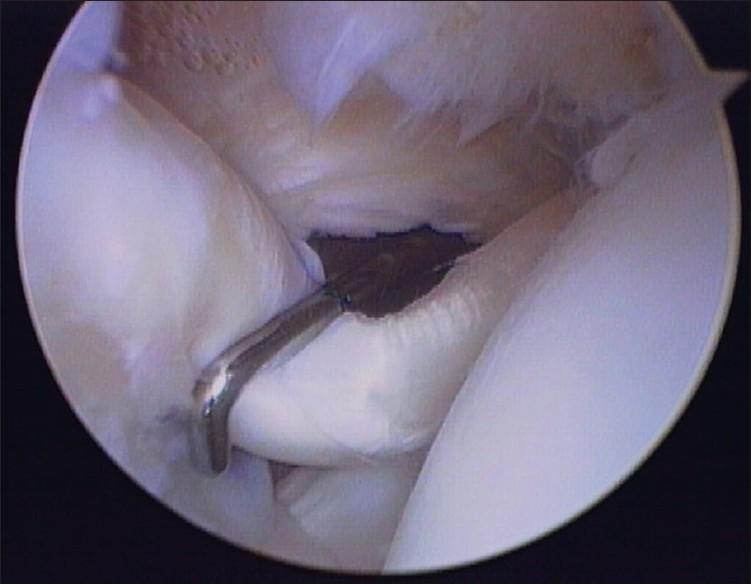 | Figure 1: Arthroscopic photograph of a Lafosse grade 0 proximal biceps tendon injury
Click here to view |
 | Figure 2: Arthroscopic photograph of a Lafosse grade 1 proximal biceps tendon injury
Click here to view |
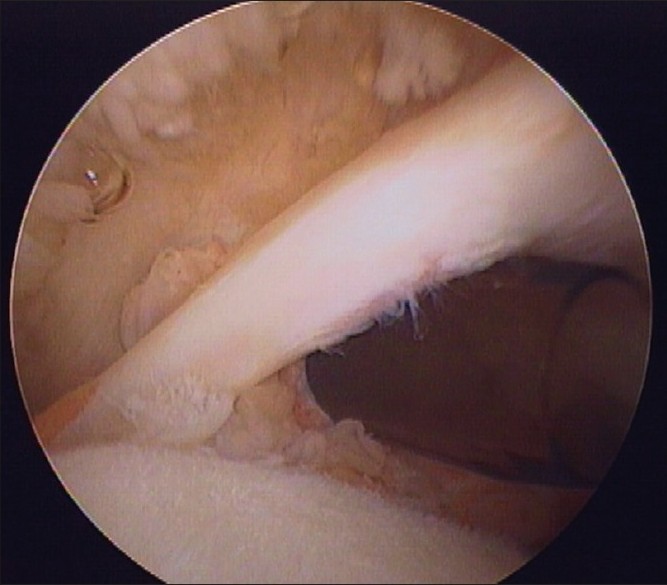
 | Figure 3: Arthroscopic photograph of a Lafosse grade 2 proximal biceps tendon injury
Click here to view |
Approximately four months after the initial survey, the same shoulder surgeons viewed the same arthroscopic videos and repeated the survey. Responses from each survey session were collected by the two primary authors and compiled for analysis. Responses of the surveyed physicians were compared with the pre-determined grading of the two primary authors.
Statistical analysis
Statistical analysis with weighted and non-weighted Kappa values was performed to determine intra- and interobserver reliability for severity grading, as also to determine the preferred treatments for each level of severity. This was performed by the certified statistics staff at our Sports Medicine Center.
| Results | | |
Patient demographics
Thirty cases of biceps tendon injuries were collected prospectively. Twenty of the patients were male, and ten were female. Twenty of the patients had symptoms of the right shoulder, while the remaining ten patients had symptoms on the left. Age of the patients ranged from 31 to 72 years (average 54.0 years).
Evaluator demographics
The 13 evaluators from the MOON Shoulder Group were made up of orthopedic surgeons with varying years of experience. Twelve of the 13 surgeons had completed fellowships in Sports Medicine, Shoulder and Elbow, or both. One surgeon was, at the time of the survey, completing a fellowship in Sports Medicine. Experience of the physicians ranged from currently in fellowship to 16 years of practice experience. The average number of years of experience beyond residency for the group was 7.8 years.
Reliability testing
On the basis of the scale of Viera et al., [5] intraobserver reliability testing for the Lafosse classification system for biceps brachii long head tendon injuries showed substantial agreement [Table 2] between the 13 evaluators after two rounds of grading (81.28%, K=0.7006). Interobserver reliability testing for the system demonstrated substantial agreement for Grade 0 (K=0.7152), fair agreement for Grade 1 (K=0.3803), and moderate agreement for Grade 2 injuries (K=0.5156).
Treatment recommendations
The evaluators' combined responses [Figure 5] recommended no surgical treatment for 95.4% of the lesions that were individually classified as grade 0 (62/65). For Grade 1 lesions, no surgical treatment was recommended in 24.1% of the cases (35/145), debridement in 38.6% of the cases (56/145), and either tenotomy or tenodesis in 37.2% of the cases (54/145). Finally, the evaluators preferred tenotomy or tenodesis for 98.3% of the Grade 2 lesions (177/180).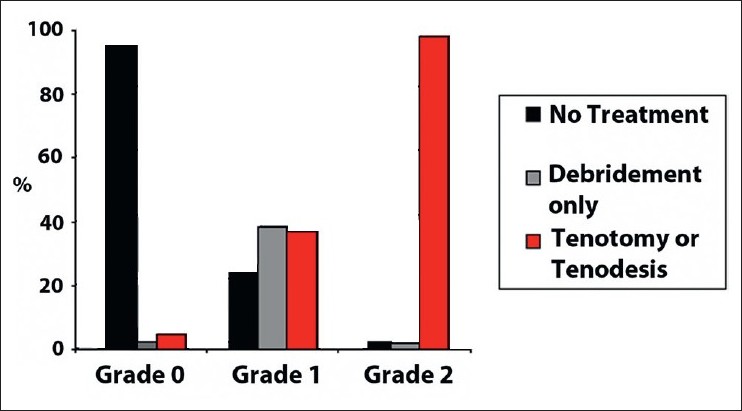 | Figure 5: Evaluators' combined responses for treatment recommendation after two rounds of grading. Results showed that 95.4% of the injuries graded as grade 0 were recommended no treatment. Evaluators recommended tenotomy or tenodesis for 98.3% of the injuries graded as grade 2
Click here to view |
| Discussion | | |
To our knowledge, no validated classification system currently exists for proximal biceps tendon injuries. A reliable classification system for these injuries is needed for standardization of treatment. The authors of this study sought to determine the inter- and intraobserver reliability of the Lafosse classification system for biceps brachii long head tendon injuries.
Results of reliability testing for the system among fellowship-trained shoulder surgeons were not favorable for the Lafosse system, with regard to interobserver reliability. Although substantial agreement was observed for Grade 0 (K=0.7152), only fair and moderate agreements were observed for Grade 1 and Grade 2, respectively (K=0.3803, 0.5156). Intraobserver reliability testing showed more favorable results with an overall K-value of 0.7006. Our results indicated that although individual evaluators were able to effectively reproduce their responses for injury grade, there was a high level of variability between evaluators for grading of the lesions.
The current study also sought to determine the ideal treatment for the varying levels of severity of these injuries. No clear treatment protocol has yet been established for lesions of the proximal biceps tendon. Results of our survey of the MOON Shoulder Group showed a clear preference for no treatment for Grade 0 lesions and tenotomy or tenodesis for Grade 2 lesions. However, given the high level of variability among the evaluators' preferred treatment for Grade 1 lesions, no clear treatment recommendation can be made for this grade.
In 2009, Frost et al. performed a systematic review of the literature with regard to the effectiveness of tenotomy versus tenodesis for the treatment of these lesions. It was determined from the study that injuries to the tendon were common, however, there was not enough literature to determine the ideal treatment. The authors of the study recommended tenotomy over tenodesis due to the relative ease of the procedure and the decreased need for postoperative rehabilitation. [6] Although not reported in the results of our study, a trend toward tenodesis was seen in the results of treatment recommendation for Grade 2 tendon lesions, but that trend was not statistically significant.
There were multiple limitations to this study. These included the relatively low power of the study. Only 30 cases were presented. Among these 30 cases, four were predetermined to be Grade 0, 11 were Grade 1, and 15 were Grade 2 on the Lafosse classification system. Also, a relatively low number of evaluators undertook the survey. Furthermore, among the evaluators, there was a wide range in years of experience in performing shoulder arthroscopy. One evaluator had not yet completed his fellowship in Sports Medicine and a second evaluator was in his first year of practice in Sports Medicine after fellowship. Also, only the static aspect of the Lafosse classification system was used for grading. This was considered necessary due to the dynamic aspect of the system requiring palpation and translation of the tendon. Finally, there were important limitations inherent to a video study. To assess the instability of the biceps, one must actively probe it and try to pull it in and out of its groove with the shoulder in different degrees of abduction and rotation. It is not practical to simulate this in a video; active manipulation is required for tactile evaluation of the biceps tendon. Our goal, however, was limited to examining the biceps tendon anatomy and to decrease the number of variables to be controlled in such an experiment.
| Conclusions | | |
Validation analysis for the Lafosse classification system for biceps tendon injuries indicates substantial intraobserver reliability for all grades. However, given that Grades 1 and 2 have shown only fair and moderate agreement, respectively, for interobserver reliability, a need for a reliable grading system still exists. Not surprisingly, no surgical procedure should be performed on the biceps tendon for Grade O lesions. Our consensus is that Grade 2 lesions should be treated with either tenotomy or tenodesis. At this time, a clear preferred treatment for Grade 1 lesions cannot be determined given the high variability of preferred treatment responses. A higher-powered survey may help to determine the ideal treatment for Grade 1 injuries in the future.
| Acknowledgement | | |
*MOON Shoulder Group contributors were Christina Allen, University of California-San Francisco; Keith Baumgarten, Orthopaedic Institute, Sioux Falls, S.D.; Julie Y. Bishop, The Ohio State University, Columbus, OH; Robert Brophy, Washington University, St. Louis, Mo.; James Carey, University of Pennsylvania, Radnor, Pa.; Charles L. Cox, Vanderbilt University, Nashville, Tenn.; Warren Dunn, Vanderbilt University, Nashville, Tenn.; Brian Holloway, Knoxville Orthopaedic Clinic, Knoxville, Tenn.; John E. Kuhn, Vanderbilt University, Nashville, Tenn.; Benjamin Ma, University of California-San Francisco; Robert Marx, Hospital for Special Surgery, New York, N.Y.; Eric McCarty, University of Colorado, Denver, Colo.; Bruce Miller, University of Michigan, Ann Arbor; Matthew V. Smith, Washington University, St. Louis, Mo.; Edwin Spencer, Knoxville Orthopaedic Clinic, Knoxville, Tenn.; Armando Vidal, University of Colorado, Denver, Colo. ; Rick W. Wright, Washington University, St. Louis, Mo.; and Brian R. Wolf, University of Iowa, Iowa City.
| References | | |
| 1. | Lafosse L, Reiland Y, Baier GP, Toussaint B, Jost B. Anterior and posterior instability of the long head of the biceps tendon in rotator cuff tears: A new classification based on arthroscopic observations. Arthroscopy 2007;23:73-80. 
[PUBMED] [FULLTEXT] |
| 2. | Bennett W. Correlation of the SLAP lesion with lesions of the medial sheath of the biceps tendon and intra-articular subscapularis tendon. Indian J Orthop 2009;43:342-6.
[PUBMED]  |
| 3. | Friedman DJ, Dunn JC, Higgins LD, Warner JJ. Proximal biceps tendon: Injuries and management. Sports Med Arthrosc 2008;16:162-9.
[PUBMED] [FULLTEXT] |
| 4. | Ghalayini SR, Board TN, Srinivasan MS. Anatomic variations in the long head of biceps: Contribution to shoulder dysfunction. Arthroscopy 2007;23:1012-8.
[PUBMED] [FULLTEXT] |
| 5. | Viera AJ, Garrett JM. Understanding interobserver agreement: The kappa statistic. J Fam Med 2005;37:360-3.
|
| 6. | Frost A, Zafar MS, Maffulli N. Tenotomy versus tenodesis in the management of pathologic lesions of the tendon of the long head of the biceps brachii. Am J Sports Med 2009;37:828-33.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
[Table 1], [Table 2]
| This article has been cited by | | 1 |
The longitudinal anatomy of the long head of the biceps tendon and implications on tenodesis |
|
| Waqas M. Hussain,Deepak Reddy,Alfred Atanda,Morgan Jones,Mark Schickendantz,Michael A. Terry | | Knee Surgery, Sports Traumatology, Arthroscopy. 2014; | | [Pubmed] | [DOI] | | | 2 |
Tenotomy or tenodesis for long head biceps lesions in shoulders with reparable rotator cuff tears: a prospective randomised trial |
|
| Qiang Zhang,Jiaojiao Zhou,Heng’an Ge,Biao Cheng | | Knee Surgery, Sports Traumatology, Arthroscopy. 2013; | | [Pubmed] | [DOI] | | | 3 |
Clinical Examination of the Rotator Cuff |
|
| Nitin B. Jain,Reg B. Wilcox,Jeffrey N. Katz,Laurence D. Higgins | | PM&R. 2013; 5(1): 45 | | [Pubmed] | [DOI] | | | 4 |
Clinical Examination of the Rotator Cuff |
|
| Jain, N.B. and Wilcox, R.B. and Katz, J.N. and Higgins, L.D. | | PM and R. 2013; 5(1): 45-56 | | [Pubmed] | |
|
|
|
|