| |


 |
| Year : 2011 | Volume
: 5
| Issue : 4 | Page : 90-94 |
|
|
|
|
|
ORIGINAL ARTICLE The frequency of subscapularis tears in arthroscopic rotator cuff repairs: A retrospective study comparing magnetic resonance imaging and arthroscopic findings
Guido Garavaglia1, Henri Ufenast2, Ettore Taverna2
1 Departement of Orthopaedics, ORBV, Bellinzona, Switzerland
2 Departement of Surgery, OBV, Mendrisio, Switzerland
Correspondence Address:
Guido Garavaglia
Servizio di Ortopedia e Traumatologia, Ospedale Regionale di Bellinzona e Valli, 6500 Bellinzona
Switzerland
 Source of Support: None, Conflict of Interest: None  | 17 |
DOI: 10.4103/0973-6042.91000

|
|
|
|
| Date of Web Publication | 20-Dec-2011 |
 Abstract Abstract | | |
Purpose: With the advent of arthroscopic shoulder surgery the comprehension and description of rotator cuff tears have strongly evolved. Subscapularis tears are difficult to recognize and are underestimated. Our purpose is to report our observations concerning the relative frequency of subscapularis tears in patients undergoing arthroscopic rotator cuff repair and to compare the arthroscopic observations with the magnetic resonance imaging (MRI) findings.
Materials and Methods: Retrospective cohort study including all patients undergoing arthroscopic rotator cuff repair was performed between March 2006 and March 2009 at our institution. Preoperative MRI findings, intraoperative arthroscopic findings, and details of surgical intervention were collected using medical charts.
Results: We reviewed the medical charts of a total of 348 consecutive arthroscopic rotator cuff repairs. There were 311 supraspinatus tears (89%), 48 infraspinatus tears (14%), and 129 subscapularis tears (37%). MRI sensitivity and specificity were respectively 0.25 and 0.98 for subscapularis tendon tears, 0.67 and 1.0 for supraspinatus tears and 0.5 and 0.99 for infraspinatus tears.
Conclusion: Subscapularis tears are frequent lesions and usually appear concomitantly with supra or infraspinatus lesions. We propose a classification of subscapularis tendon tears, based on our observations of the pathoanatomy of the tears. While concordance with MRI results are good for the supraspinatus, MRI often fails to diagnose the presence of subscapularis tears and infraspinatus tears
Keywords: Classification of subscapularis tears, rotator cuff, shoulder arthroscopy, subscapularis tendon
How to cite this article:
Garavaglia G, Ufenast H, Taverna E. The frequency of subscapularis tears in arthroscopic rotator cuff repairs: A retrospective study comparing magnetic resonance imaging and arthroscopic findings. Int J Shoulder Surg 2011;5:90-4 |
How to cite this URL:
Garavaglia G, Ufenast H, Taverna E. The frequency of subscapularis tears in arthroscopic rotator cuff repairs: A retrospective study comparing magnetic resonance imaging and arthroscopic findings. Int J Shoulder Surg [serial online] 2011 [cited 2016 Apr 25];5:90-4. Available from: http://www.internationalshoulderjournal.org/text.asp?2011/5/4/90/91000 |
| Introduction | |  |
With the advent of arthroscopic shoulder surgery our understanding of pathological conditions of the shoulder is improving. The comprehension and description of rotator cuff tears have strongly evolved. Although magnetic resonance imaging (MRI) has shown to be a useful tool for the diagnosis of supraspinatus and infraspinatus tendon tears, [1],[2],[3],[4],[5],[6] we believe that subscapularis tendon tears are more difficult to recognize and are therefore underestimated. The prevalence of subscapularis tendon tears has not been widely studied, [7],[8] and only a few authors have classified them. [7],[9] To the best of our knowledge, no study to date has compared MRI findings with arthroscopic findings based on the same classification. Thus, the purpose of our study is to report our observations concerning the relative frequency of subscapularis tears in patients undergoing arthroscopic rotator cuff repair, to propose a modification of the existing classifications, and to compare the arthroscopic observations with the MRI findings.
| Materials and Methods | | |
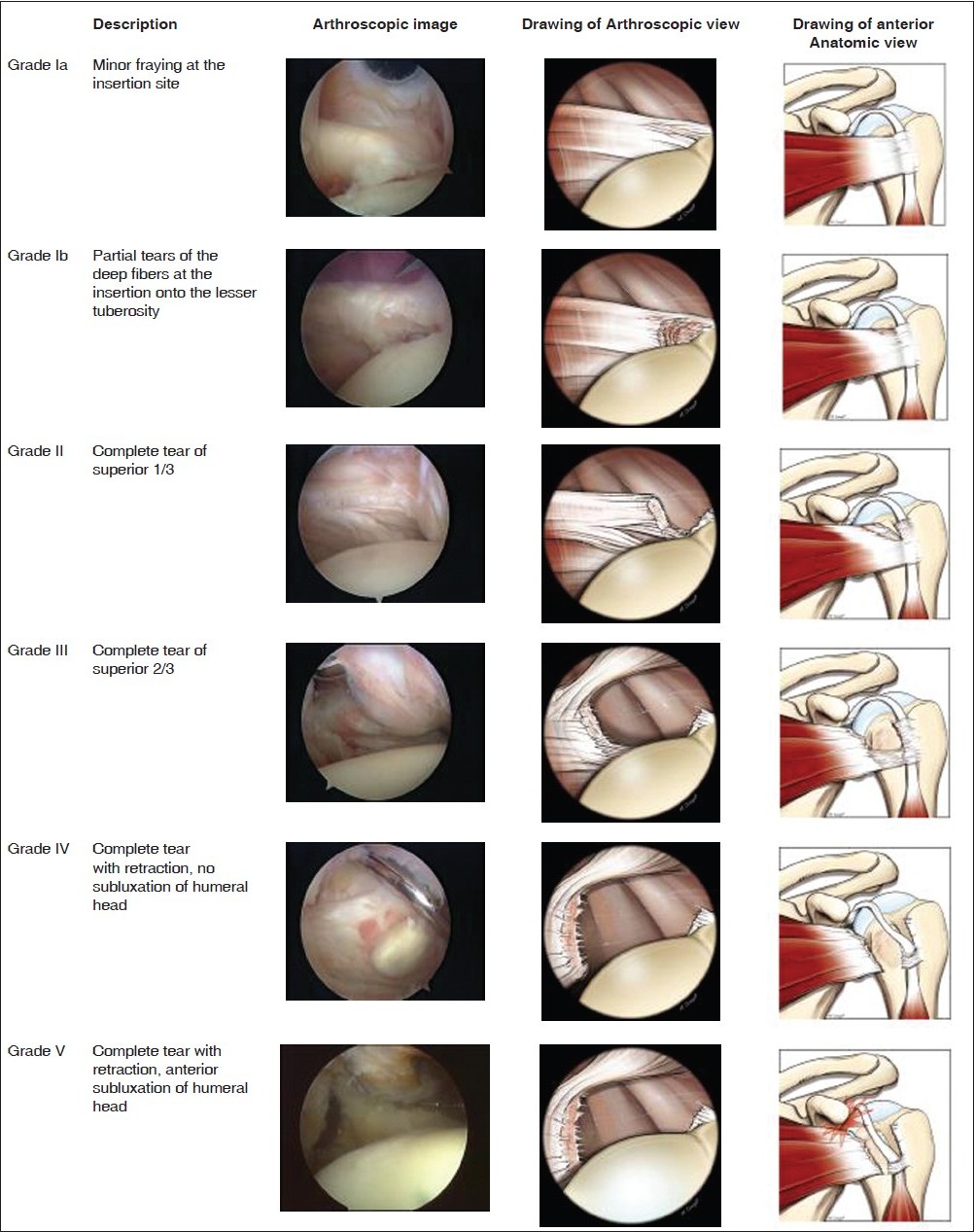
We performed a retrospective cohort study including all patients who underwent arthroscopic rotator cuff repair between March 2006 and March 2009 at our institution. All interventions were performed by the three senior authors. Using medical charts and pictures as well as recorded video sequences, we collected information concerning intraoperative arthroscopic findings and details of surgical interventions. We then counted the number of supraspinatus, infraspinatus, and subscapularis tendon tears. For subscapularis tears, we noted the type of lesion according to the classification proposed by Lafosse et al. [7] We have modified the classification by introducing a distinction for superior third partial lesions (grade I), distinguishing two subgroups: grade Ia lesions show only minor fraying at the insertion site and grade Ib lesions present partial tears of the posterior deep fibers at the insertion onto the lesser tuberosity [Figure 1].
The number of performed associated procedures, such as tenotomy or tenodesis of the long head of the biceps (LHB), subacromial decompression, and acromioclavicular joint resections were also recorded.
The preoperative MRI findings as described by the radiologist, when available, were collected and compared with the intraoperative findings.
Arthroscopic technique
Patients underwent regional anesthesia with an interscalene block or general anesthesia with a laryngeal mask. Our standard arthroscopic examination is as follows: The patient is placed in the beach chair position without traction. The scope is introduced through a standard posterior portal and glenohumeral inspection is started from the LHB origin. Its intra-articular and intertubercular course is assessed with a probe inserted through an anterior--inferior portal. After examination of the LHB, the articular side of the subscapularis and supraspinatus tendons is inspected. For the inspection of the subscapularis tendon, the arm is positioned with 30° abduction and 30° external rotation. Only with the arm in this position is it possible to observe the insertion of the deep fibers of the subscapularis tendon on the lesser tuberosity. If there is any doubt about tendon integrity because of synovitis and/or scar tissue at its insertion, a careful debridement is performed and the tendon insertion is reassessed using a probe. If a subscapularis tendon tear is detected, we repair the tendon with an intra-articular technique. Subscapularis tendon repair is usually combined with either LHB tenotomy or tenodesis, depending on age and functional requirements of the patient. We therefore place a supplemental lateral portal precisely in line with the bicipital groove. The footprint of the subscapularis tendon is prepared and the tendon is freed from any adherence. A double-loaded titanium suture anchor is placed in the footprint. We grasp the tendon through the lateral approach aligned with the tendon fibers. The sutures are then passed through the tendon using a 10° upward penetrating instrument. Finally, the tendon is reinserted on its footprint with two vertical sutures using sliding knots.
The scope is then reintroduced in the subacromial space. Bursectomy is performed if needed. Then we turn our attention to the superior and posterior cuff. If a tear is present, we repair the tendon using different configurations of repair, depending on size, retraction, and geometry of the tear.
| Results | | |
We reviewed the medical charts of a total of 348 consecutive arthroscopic rotator cuff repairs. Mean age was 56 years (78-23), with 151 females and 197 males. There were 311 supraspinatus tears (89%), 48 infraspinatus tears (14%), and 129 subscapularis tears (37%) [Figure 2]. In 5 patients (1.4%), the subscapularis tear was isolated. The frequencies of the different types of subscapularis tendon lesions are shown in [Figure 3].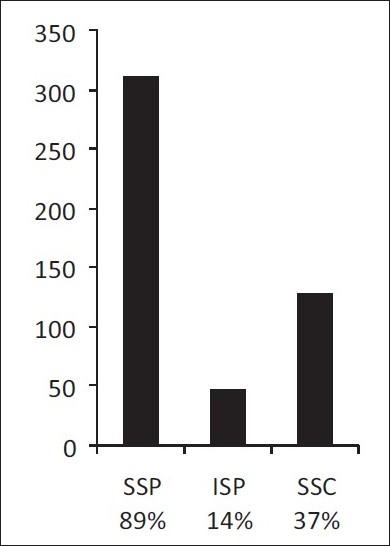 | Figure 2: Relative frequency of rotator cuff tendon tears found during 348 consecutive shoulder arthroscopies ( SSP = Supraspinatus, ISP = Infraspinatus, SSC = Subscapularis)
Click here to view |
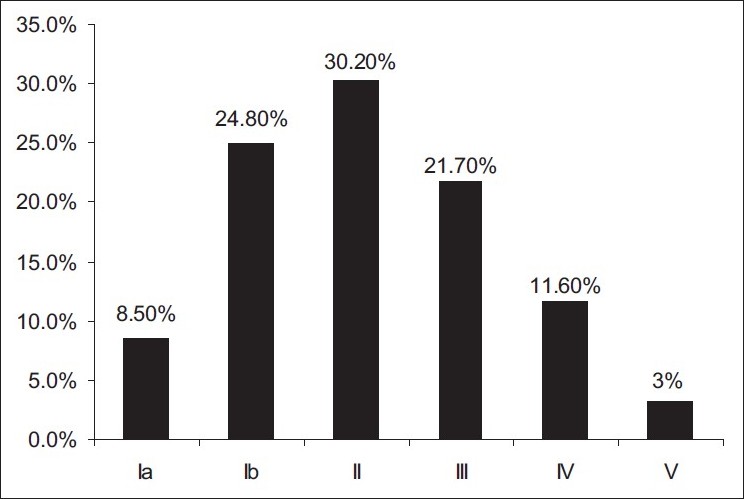 | Figure 3: Relative frequency of different types of subscapularis tendon lesions
Click here to view |
Subacromial decompressions were performed in 245 cases (70%), acromioclavicular resections in 19 cases (5%), and in 280 cases (80%) a biceps tenodesis or tenotomy was performed because of either instability or degeneration of the tendon.
The MRI report written by the radiologist was available in 213 cases and compared to the intraoperative findings [Table 1].
| Discussion | | |
The most interesting finding in our study was the elevated frequency of arthroscopically established subscapularis tears (37%) compared to the documented MRI findings (sensitivity of 0.25).
The prevalence of subscapularis tendon tears has not been widely studied. Kim et al. [8] reported 19% of subscapularis tendon tears found during arthroscopic procedures of 314 consecutive shoulders.
In a study concerning the outcome of arthroscopic repair of isolated subscapularis tendon tears, Lafosse et al. [7] reported a total of 169 subscapularis tears in 342 rotator cuff repairs (49.4%). They found a prevalence of isolated subscapularis tears of 10.1% and using their classification they documented 2.9% of grade I lesions, 27.8% of grade II lesions, and 18.7% of grade III and IV lesions.
In our series we found 37% of subscapularis tears during 348 consecutive shoulder arthroscopies performed for rotator cuff pathology. Our results are therefore between those reported by Kim et al. [8] and Lafosse et al. [7] In comparison to the series reported by Kim et al, [8] our higher incidence of subscapularis tears is certainly explainable by the fact that we only included arthroscopies performed for rotator cuff pathologies, while in their study they also considered arthroscopies performed for other pathologies such as instability.
Grade I lesions accounted for one third of all subscapularis tendon lesions, constituting a considerable number of cases and a potential source of residual complaints if not addressed during rotator cuff surgery. Most of our grade I and grade II lesions were associated with an anterosuperior lesion of the rotator cuff, involving a pulley lesion and a lesion of the anterior portion of the supraspinatus. [10] Grade III and grade V lesions were mostly seen in the presence of large supraspinatus lesions. In these cases the diagnosis of the rupture is often straightforward, but finding the remnant subscapularis tendon can be technically difficult. We always preserve the 'comma sign' and use it as a guide to identify the tendon. [11],[12] Most cases in which the preoperative clinical suspicion of a subscapularis tear was confirmed intraoperatively presented a grade III or IV lesion. In contrast, the smaller grade I and II subscapularis lesions were often not recognized preoperatively.
There are several studies showing that MRI is accurate for the detection of abnormalities of the rotator cuff. [1-6] Most studies, however, have focused on supraspinatus tendon lesions, and little attention has been paid to disorders of the subscapularis. Pfirrmann et al. [13] showed that a good diagnostic accuracy could be obtained using transverse images on MRI arthrography, also for detection and grading of subscapularis tendon lesions. They emphasized the importance of associating the findings of the transverse and parasagittal images to indirect signs such as contrast medium leakage or abnormalities in the course of the long biceps tendon.
In rotator cuff pathologies, there is a great variation in the reported MRI findings in the literature, with sensitivity values ranging from 0.41 to 1.0 and specificity from 0.79 to 1.0. [3] The results obtained in our study are therefore in the range reported in the literature for supraspinatus lesions, while the results obtained for the detection of subscapularis tendon lesions show a much lower accuracy. We are aware that numerous variables may affect our results, since MRI examinations were performed in five different institutions by using different imaging protocols and often interpreted by different radiologists. Nevertheless, we believe that grade Ia, Ib, and II lesions of the subscapularis tendon are difficult to detect on MRI scans, especially in the absence of indirect signs.
Despite the advances made using MRI for the detection of rotator cuff tears and the refinements in clinical examination tests, lesions of the subscapularis tendon are still an underdiagnosed condition. [7]
Several studies have shown that the diagnostic accuracy of individual physical examination tests is limited. For the subscapularis tendon, different clinical tests have been described and although some might be useful in raising suspicion about a possible abnormality of the tendon, both sensitivity and specificity of the tests remain low. [14],[15]
Even with arthroscopy, the recognition of subscapularis tendon lesions can be difficult because of the incomplete visualization of its insertion at the lesser tuberosity. [16],[17] Synovitis and/or scar tissue at the tendon insertion, inadequate arthroscopic portals, or inadequate arm position during the intra-articular inspection can hide the real insertion of the tendon on the lesser tuberosity. Partial tears of the superior third of the subscapularis (grade Ia and Ib) are missed if this area is not properly visualized and if the arthroscopic pathoanatomy of these lesions is not completely understood. [10],[17],[18]
In contrast to the existing classifications, [7],[9] we think it is important to differentiate partial lesions of the superior third in grade Ia and Ib lesions. If there is no detachment of the fibers from the footprint (grade Ia), a debridement of the lesion alone is sufficient. If there is a detachment of the deep fibers, a repair is usually necessary.
The limitations of this study are as follows: first, it is a retrospective cohort study, and second, there might be an overreporting bias in the subjective intraoperative findings. Furthermore, we did not record the number and type of associated biceps pulley lesions. Therefore, further reports in the literature are certainly necessary to corroborate our findings. Nonetheless, our principal goal is to present our observations about the high prevalence of subscapularis lesions and we suggest a modification of the existing classifications [7],[9] as we believe that a more detailed description of superior third partial lesions is essential for the recognition of these lesions and their treatment.
| References | | |
| 1. | De Jesus JO, Parker L, Frangos AJ, Nazarian LN. Accuracy of MRI, MR arthrography, and ultrasound in the diagnosis of rotator cuff tears: a meta-analysis. AJR Am J Roentgenol 2009;192:1701-7. 
|
| 2. | Kuhn JE, Dunn WR, Ma B, Wright RW, Jones G, Spencer EE, et al. Interobserver agreement in the classification of rotator cuff tears. Am J Sports Med 2007;35:437-41.
|
| 3. | Quinn SF, Sheley RC, Demlow TA, Szumowski J. Rotator cuff tendon tears: Evaluation with fat-suppressed MR imaging with arthroscopic correlation in 100 patients. Radiology 1995;195:497-500.
|
| 4. | Schröder RJ, Bostanjoglo M, Kääb M, Herzog H, Hidajat N, Röttgen R, et al. Accuracy of routine MRI in lesions of the supraspinatus tendon--comparison with surgical findings. Rofo 2003;175:920-8.
|
| 5. | Theodoropoulos JS, Andreisek G, Harvey EJ, Wolin P. Magnetic resonance imaging and magnetic resonance arthrography of the shoulder: Dependence on the level of training of the performing radiologist for diagnostic accuracy. Skeletal Radiol 2010;39:661-7.
|
| 6. | Waldt S, Bruegel M, Mueller D, Holzapfel K, Imhoff AB, Rummeny EJ, et al. Rotator cuff tears: Assessment with MR arthrography in 275 patients with arthroscopic correlation. Eur Radiol 2007;17:491-8.
|
| 7. | Lafosse L, Jost B, Reiland Y, Audebert S, Toussaint B, Gobezie R. Structural integrity and clinical outcomes after arthroscopic repair of isolated subscapularis tears. J Bone Joint Surg Am 2007;89:1184-93.
|
| 8. | Kim TK, Rauh PB, McFarland EG. Partial tears of the subscapularis tendon found during arthroscopic procedures on the shoulder: A statistical analysis of sixty cases. Am J Sports Med 2003;31:744-50.
|
| 9. | Fox JA, Noerdlinger MA, Romeo AA. Operative arthroscopic subscapularis repair. Tech Orthop, 2002;12:209-17.
|
| 10. | Habermeyer P, Magosch P, Pritsch M, Scheibel MT, Lichtenberg S. Anterosuperior impingement of the shoulder as a result of pulley lesions: A prospective arthroscopic study. J Shoulder Elbow Surg 2004;13:5-12.
|
| 11. | Burkhart SS, Brady PC. Arthroscopic subscapularis repair: Surgical tips and pearls A to Z. Arthroscopy 2006;22:1014-27.
|
| 12. | Lo IK, Burkhart SS. The comma sign: An arthroscopic guide to the torn subscapularis tendon. Arthroscopy 2003;19:334-7.
|
| 13. | Pfirrmann CW, Zanetti M, Weishaupt D, Gerber C, Hodler J. Subscapularis tendon tears: detection and grading at MR arthrography. Radiology 1999;213:709-14.
|
| 14. | Beaudreuil J, Nizard R, Thomas T, Peyre M, Liotard JP, Boileau P, et al. Contribution of clinical tests to the diagnosis of rotator cuff disease: a systematic literature review. Joint Bone Spine 2009;76:15-9.
|
| 15. | Hegedus EJ, Goode A, Campbell S, Morin A, Tamaddoni M, Moorman CT 3 rd , et al. Physical examination tests of the shoulder: A systematic review with meta-analysis of individual tests. Br J Sports Med 2008;42:80-92.
|
| 16. | David TS, Bravo H, Scobercea R. Arthroscopic visualization of subscapularis tendon lesions. Orthopedics. 2009 Sep;32(9). pii: orthosupersite.com/view.asp?rID=43203. doi: 10.3928/01477447-20090728-38.
|
| 17. | Wright JM, Heavrin B, Hawkins RJ, Noonan T. Arthroscopic visualization of the subscapularis tendon. Arthroscopy 2001;17:677-84.
|
| 18. | D'Addesi LL, Anbari A, Reish MW, Brahmabhatt S, Kelly JD. The subscapularis footprint: an anatomic study of the subscapularis tendon insertion. Arthroscopy 2006;22:937-40.
|
[Figure 1], [Figure 2], [Figure 3]
[Table 1]
| This article has been cited by | | 1 |
The diagnostic value of magnetic resonance imaging for different types of subscapularis lesions |
|
| Lin Lin,Hui Yan,Jian Xiao,Zhenming He,Hao Luo,Xu Cheng,Yingfang Ao,Guoqing Cui | | Knee Surgery, Sports Traumatology, Arthroscopy. 2014; | | [Pubmed] | [DOI] | | | 2 |
Diagnostic accuracy of magnetic resonance imaging for subscapularis tendon tears using radial-slice magnetic resonance images |
|
| Ryuhei Furukawa,Toru Morihara,Yuji Arai,Hirotoshi Ito,Yoshikazu Kida,Tsuyoshi Sukenari,Motoyuki Horii,Kazuya Ikoma,Hiroyoshi Fujiwara,Toshikazu Kubo | | Journal of Shoulder and Elbow Surgery. 2014; | | [Pubmed] | [DOI] | | | 3 |
Sensitivity of Physical Examination Versus Arthroscopy in Diagnosing Subscapularis Tendon Injury |
|
| Sami Faruqui,Coen Wijdicks,Abdullah Foad | | Orthopedics. 2014; 37(1): e29 | | [Pubmed] | [DOI] | | | 4 |
Internal rotation resistance test at abduction and external rotation: a new clinical test for diagnosing subscapularis lesions |
|
| Lin Lin,Hui Yan,Jian Xiao,Yingfang Ao,Guoqing Cui | | Knee Surgery, Sports Traumatology, Arthroscopy. 2013; | | [Pubmed] | [DOI] | | | 5 |
Arthroscopic repair of subscapularis tears: Preliminary data from a prospective multicentre study |
|
| B. Toussaint,S. Audebert,J. Barth,C. Charousset,A. Godeneche,T. Joudet,Y. Lefebvre,L. Nove-Josserand,E. Petroff,N. Solignac,P. Hardy,C. Scymanski,C. Maynou,C.-E. Thelu,P. Boileau,M. Pitermann,N. Graveleau | | Orthopaedics & Traumatology: Surgery & Research. 2012; 98(8): S193 | | [Pubmed] | [DOI] | | | 6 |
New endoscopic classification for subscapularis lesions |
|
| B. Toussaint,J. Barth,C. Charousset,A. Godeneche,T. Joudet,Y. Lefebvre,L. Nove-Josserand,E. Petroff,N. Solignac,P. Hardy,C. Scymanski,C. Maynou,C.-E. Thelu,P. Boileau,N. Graveleau,S. Audebert | | Orthopaedics & Traumatology: Surgery & Research. 2012; 98(8): S186 | | [Pubmed] | [DOI] | | | 7 |
Nouvelle classification endoscopique des lésions du sub-scapulaire |
|
| B. Toussaint,J. Barth,C. Charousset,A. Godeneche,T. Joudet,Y. Lefebvre,L. Nove-Josserand,E. Petroff,N. Solignac,P. Hardy,Christophe Scymanski,C. Maynou,C.-E. Thelu,P. Boileau,N. Graveleau,S. Audebert | | Revue de Chirurgie Orthopédique et Traumatologique. 2012; 98(8): S419 | | [Pubmed] | [DOI] | | | 8 |
Réparation arthroscopique du sous-scapulaire : résultats préliminaires d’une étude prospective multicentrique |
|
| B. Toussaint,S. Audebert,J. Barth,C. Charousset,A. Godeneche,T. Joudet,Y. Lefebvre,L. Nove-Josserand,E. Petroff,N. Solignac,P. Hardy,C. Scymanski,C. Maynou,C.-E. Thelu,P. Boileau,M. Pitermann,N. Graveleau | | Revue de Chirurgie Orthopédique et Traumatologique. 2012; 98(8): S427 | | [Pubmed] | [DOI] | | | 9 |
Arthroscopic repair of subscapularis tears: Preliminary data from a prospective multicentre study |
|
| Toussaint, B. and Audebert, S. and Barth, J. and Charousset, C. and Godeneche, A. and Joudet, T. and Lefebvre, Y. and Nove-Josserand, L. and Petroff, E. and Solignac, N. and Hardy, P. and Scymanski, C. and Maynou, C. and Thelu, C.-E. and Boileau, P. and Pitermann, M. and Graveleau, N. | | Orthopaedics and Traumatology: Surgery and Research. 2012; 98(8 SUPPL): S193-S200 | | [Pubmed] | | | 10 |
Arthroscopic repair of subscapularis tears: Preliminary data from a prospective multicenter study [Réparation arthroscopique du sous-scapulaire : Résultats préliminaires dæune étude prospective multicentrique] |
|
| Toussaint, B. and Audebert, S. and Barth, J. and Charousset, C. and Godeneche, A. and Joudet, T. and Lefebvre, Y. and Nove-Josserand, L. and Petroff, E. and Solignac, N. and Hardy, P. and Scymanski, C. and Maynou, C. and Thelu, C.-E. and Boileau, P. and Pitermann, M. and Graveleau, N. | | Revue de Chirurgie Orthopedique et Traumatologique. 2012; 98(SUPPL. 8): S427-S435 | | [Pubmed] | | | 11 |
New endoscopic classification for subscapularis lesions |
|
| Toussaint, B. and Barth, J. and Charousset, C. and Godeneche, A. and Joudet, T. and Lefebvre, Y. and Nove-Josserand, L. and Petroff, E. and Solignac, N. and Hardy, P. and Scymanski, C. and Maynou, C. and Thelu, C.-E. and Boileau, P. and Graveleau, N. and Audebert, S. | | Orthopaedics and Traumatology: Surgery and Research. 2012; 98(8 SUPPL): S186-S192 | | [Pubmed] | |
|
|
|


|
|
|
|
|