| |


 |
| Year : 2013 | Volume
: 7
| Issue : 3 | Page : 120-123 |
|
|
|
|
|
SURGICAL TECHNIQUE Arthroscopically assisted Latarjet procedure: A new surgical approach for accurate coracoid graft placement and compression
Ettore Taverna1, Henri Ufenast1, Laura Broffoni1, Guido Garavaglia2
1 Upper Limb Unit, Department of Surgery, OBV, Mendrisio, Switzerland
2 Department of Orthopaedics and Trauma Surgery, ORBV, Bellinzona, Switzerland
Correspondence Address:
Guido Garavaglia
Department of Orthopaedics and Trauma Surgery, ORBV 6500 Bellinzona
Switzerland
 Source of Support: None, Conflict of Interest: None  | 3 |
DOI: 10.4103/0973-6042.118912

|
|
|
|
| Date of Web Publication | 25-Sep-2013 |
 Abstract Abstract | | |
The Latarjet procedure is a confirmed method for the treatment of shoulder instability in the presence of bone loss. It is a challenging procedure for which a key point is the correct placement of the coracoid graft onto the glenoid neck. We here present our technique for an athroscopically assisted Latarjet procedure with a new drill guide, permitting an accurate and reproducible positioning of the coracoid graft, with optimal compression of the graft onto the glenoid neck due to the perfect position of the screws: perpendicular to the graft and the glenoid neck and parallel between them.
Keywords: Glenoid bone loss, Latarjet procedure, shoulder instability
How to cite this article:
Taverna E, Ufenast H, Broffoni L, Garavaglia G. Arthroscopically assisted Latarjet procedure: A new surgical approach for accurate coracoid graft placement and compression. Int J Shoulder Surg 2013;7:120-3 |
| Introduction | |  |
The effectiveness of the Latarjet procedure for the treatment of anterior glenohumeral instability has been extensively reported. [1],[2],[3],[4] Since, the description of the original technique by Latarjet, [5] many modifications have been proposed and recently the procedure has been performed arthroscopically. [6],[7] Successful treatment clearly depends on proper patient selection and pre-operative evaluation, but for the procedure itself one of the most important details is an accurate placement of the coracoid graft. [4],[8],[9] Besides the correct positioning of the graft onto the glenoid neck, in order to obtain the best compression between the graft and the glenoid, it is of paramount importance that the screws are placed parallel to each other and perpendicular to the glenoid neck.
We would like to present our technique for an arthroscopically-assisted Latarjet procedure with a new drill guide. The new drill guide ( TM Smith and Nephew) permits precise positioning under arthroscopic control of two sleeves into the glenoid and therefore, allows a perfect positioning of the screws and optimal fixation of the coracoid graft.
| Surgical Technique | | |
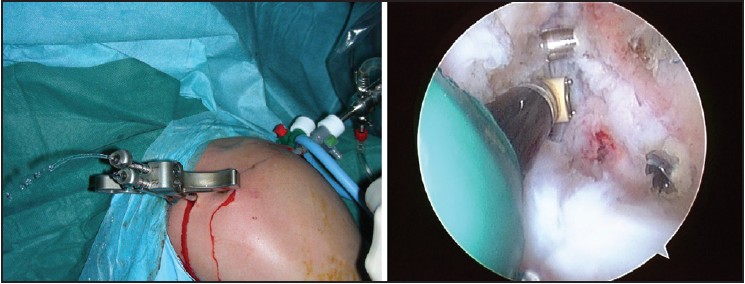
Patient positioning
We always perform the procedure positioning the patient in the beach chair position. Draping allows ready access to the posterior and anterior aspects of the shoulder girdle and the arm is draped free to allow intra-operative mobilization.
Portals and intra-articular preparation
A high posterior lateral viewing portal is preferred for initial glenohumeral inspection so as to allow a subsequent posterior vector guide and double barrel guide sleeve to be inserted posteriorly into the joint. Standard anterior superior and mid-glenoid portals are made by means of 5.5 mm and 7.0 mm cannulas.
Following joint inspection, the anterior labrum and capsule are detached from the anterior rim of the glenoid by means of the combination of an elevator, shaver, and radio frequency device. The capsulo-labral complex is freed to view the subscapularis muscle fibers. The anterior bony glenoid defect is then smoothed and freshened with a motorized bur.
If the capsule and ligament consistency is satisfactory, we place 1-3 soft anchors completely suture-based passing the sutures through the capsule and ligaments, in preparation for the anterior capsular reconstruction, which we perform by tying the knots only after fixation of the coracoid on the anterior glenoid neck.
The drill guide
The drill guide consists of an ergonomic handle with an arm with a hook at the extremity. Two pins permit to guide the drill sleeves with a central drill bit. The drill is therefore a two piece combination of a small diameter drill bit attached to a small cannula sleeve (drill sleeve). Its maximum diameter equals a pre-tapped hole for a 4 mm screw (2.7 mm). Once in position the pin rests against the posterior glenoid neck while the drill sleeve and the central drill bit protrude from the anterior cortex [Figure 1]. | Figure 1: The drill guide consists of a handle with an arm with a hook at the extremity. Two pins permit to guide the drill sleeves with a central drill bit
Click here to view |
The drill sleeve and drill bit combination are used to create an accessible posterior to anterior pilot hole in the glenoid, which is used to carry out procedural steps including passage of guidewires for coracoid guidance and temporary placement, cannulated screw guidance and final fixation. The sleeve itself is removed before the introduction of the screw in the pre-drilled glenoid, the guidewires are kept in place until final fixation of the screw.
Drill guide placement
A spinal needle is inserted posteriorly and brought to rest against the face of the glenoid south of the equator and centered on the anterior glenoid defect. A second posterior portal is created and the drill guide is inserted posteriorly and its arm placed flush along the face of the glenoid with its hook passed over the edge of the glenoid [Figure 2]. Each pin of the guide is then advanced until it rests against the posterior glenoid neck and the drill sleeves with a central drill bit are inserted and advanced under power until they exit 4 mm medial to the cortical margin of anterior glenoid, measured from the center of the hole [Figure 3].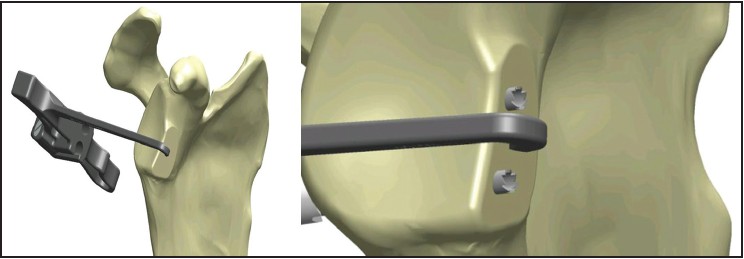 | Figure 2: The drill guide is placed with the tip over the bony defect and the arm flush along the face of the glenoid
Click here to view |
 | Figure 3: The drill guide with the two pins are placed under arthroscopic control: The drill sleeves and the central drill bit are advanced until they protrude 4 mm medial to the cortical margin of anterior glenoid
Click here to view |
It is important to identify the cortex from the articular cartilage to ensure proper depth placement of the sleeves. The correct screw length can be read on the graduated sleeves as they posteriorly protrude from the guide pins. At this point, two drill sleeves are parallel to the glenoid face and to one other as well as perpendicular to the glenoid neck. We then remove the scope and the cannulas and proceed with the open part of the procedure.
Arthrotomy
We perform the open part of the procedure as described by Young et al. [4] using a limited deltopectoral approach, incorporating the mid glenoid portal at the top of the incision. After having performed the coracoid osteotomy, the inferior surface is prepared by removing the soft-tissue and a layer of cortical bone by using the saw, thus creating a flat surface of bleeding bone. At this point, using the 2.7 drill bit a single drill hole is made at about 5 mm from the apex, in the central axis of the coracoid. Since, the usual width of the coracoid is about 10 mm, drilling the hole in the central axis permits to place the coracoid flush with the glenoid bony margin. In big patients with a coracoid of more than 10 mm of width, the hole should be drilled eccentrically at 4-5 mm from the lateral edge.
For the glenoid exposure, we perform a subscapularis split at the junction between the superior 2/3 and the inferior 1/3. The previously prepared capsulo-labral complex is then identified and if necessary, we complete the detachment from the bone, taking care not to damage the sutures previously placed through the capsule. The glenoid is then exposed using a Fukuda retractor and two Hohman retractors placed superiorly and inferiorly.
Graft placement
A flexible metallic guide wire is then introduced posteriorly into the superior sleeve and pushed anteriorly. We then pass the coracoid and the conjoint tendon through the subscapularis split and places the graft with the freshened surface in front of the glenoid neck. The flexible guide wire is introduced in the previously pre-drilled coracoid hole and a 4.0 mm partially threaded cannulated screw is placed through the superior coracoid hole. After removal of the superior sleeve and still under the guidance of the flexible guide wire, we introduce the screw in the glenoid and fix the coracoid onto the glenoid neck. After the superior screw is positioned, we remove the superior guidewire. By not completely tightening the first screw, the coracoid can be rotated into the chosen position, we then pass a second guide wire through the inferior sleeve, in order to penetrate the glenoid and the coracoid from posterior to anterior. With the second guidewire in place, we drill the inferior coracoid hole over the guidewire. The inferior sleeve is also removed and a second cannulated partially threaded 4.0 mm screw is placed over the guidewire.
Using the guidance of the wires that pass through the sleeves, we are able to fix the coracoid flush to the glenoid, compressed by two screws perfectly parallel to each other and both perpendicular to the glenoid neck.
At this point we, re-insert the labrum, capsule, and ligaments onto the glenoid rim, retrieving the suture limbs through the subscapularis split and tying the knots of the previously implanted soft anchors completely suture-based. In this way, the coracoid and the conjoined tendon remain as extra-articular stabilizers.
Post-operative rehabilitation
The arm is placed in a standard protective sling for 3 weeks, but passive and active-assisted range-of-motion exercices are begun immediately after discharge, which is usually at day 2 or 3. External rotation is limited to 30° during the 1 st month and strengthening exercises are begun after 6 weeks. Return to sports is permitted after 3 month.
| Discussion | | |
Accurate positioning of the coracoid graft along and flush with the glenoid rim is one of the most important steps in the Latarjet procedure; concurrently achieving a perfect screw placement and graft fixation is also the most difficult part of the intervention. Obtaining adequate exposure of the glenoid can be challenging especially in young, muscular patients. Although, good results have been reported and the Latarjet procedure has become the gold standard for treatment of anterior glenohumeral instability in the presence of glenoid bone loss, [1],[2],[3],[4] concern has been raised about the possible complications associated with the procedure. [8],[10] Graft or hardware malpositioning can cause joint impingement and articular damage if too lateral, or may prove inefficient for stabilizing the joint if placed too medially.
Accurate screw and graft placement is therefore of paramount importance in order to avoid complications. [8],[9],[10] Furthermore, we believe that in order to promote graft integration and to reduce graft osteolysis the screws must be placed precisely parallel to each other and perpendicular to the coracoid graft and glenoid neck; thus, obtaining maximal inter-fragmentary compression.
Meyer et al. [9] recently reported the development of a similar drill guide with the same motivations. We believe that our technique has several advantages: First of all, the arthroscopic placement of the sleeves is a safe and reliable technique, which avoids extensive exposure. Secondly, the use of arthroscopically positioned sleeves permits an easier and even more precise placement of the coracoid graft by drilling the inferior hole once the graft is already partially fixed by the superior screw. This permits to rotate the graft into the chosen position and to drill the hole only when the mediolateral position has been verified. We never had to change the position of the superior screw. We also believe that arthroscopic preparation of the glenoid rim and the capsulo-labral reconstruction can be achieved more precisely by arthroscopy.
The described technique has so far been used for 8 cases; Computed Tomography was performed for 6 cases and standard X-rays only for 2, in all cases screws and graft were placed according to the above described principles [Figure 4]. Operative time was about 90 min and there were no perioperative complications. Shoulder swelling from the arthroscopic preparation did not create difficulties for arthrotomy and there was no need to increase the length of the incision. We never encountered any malpositioning of the drill sleeves; although, we once had to slightly change their position because of a conflict with suture anchors from a previous intervention. Furthermore, maximum attention must be paid to the correct positioning of the posterior portal for the introduction of the drill guide. If the arm of the drill guide is not parallel to the glenoid face, the drill sleeves can be malpositioned. Drilling should always be performed under arthroscopic control so that drilling can be stopped as soon as the tip of the drill is seen at the anterior cortex. If these principles are respected there is no risk of sleeve malpositioning or neurovascular injury.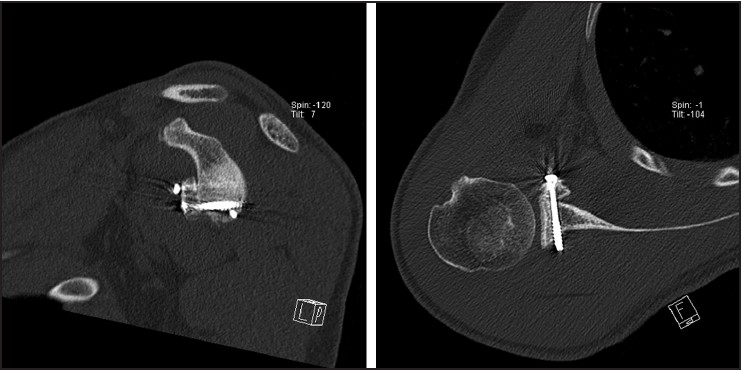 | Figure 4: Computed tomography-scan demonstrating perfect placement of screws and coracoid graft. Screws are parallel between each other, perpendicular to the graft and glenoid neck
Click here to view |
| References | | |
| 1. | Allain J, Goutallier D, Glorion C. Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder. J Bone Joint Surg Am 1998;80:841-52. 
|
| 2. | Edwards TB, Walch G. The Latarjet procedure for recurrent anterior shoulderinstability: Rationale and technique. Oper Tech Sports Med 2002;10:25-32.
|
| 3. | Schmid SL, Farshad M, Catanzaro S, Gerber C. The Latarjet procedure for the treatment of recurrence of anterior instability of the shoulder after operative repair: A retrospective case series of forty-nine consecutive patients. J Bone Joint Surg Am 2012;94:e75.
|
| 4. | Young AA, Maia R, Berhouet J, Walch G. Open Latarjet procedure for management of bone loss in anterior instability of the glenohumeral joint. J Shoulder Elbow Surg 2011;20 Suppl 2:S61-9.
|
| 5. | Latarjet M. Technic of coracoid preglenoid arthroereisis in the treatment of recurrent dislocation of the shoulder. Lyon Chir 1958;54:604-9.
|
| 6. | Lafosse L, Lejeune E, Bouchard A, Kakuda C, Gobezie R, Kochhar T. The arthroscopic Latarjet procedure for the treatment of anterior shoulder instability. Arthroscopy 2007;23:1242.e1-5.
|
| 7. | Boileau P, Bicknell RT, El Fegoun AB, Chuinard C. Arthroscopic Bristow procedure for anterior instability in shoulders with a stretched or deficient capsule: The "belt-and-suspenders" operative technique and preliminary results. Arthroscopy 2007;23:593-601.
|
| 8. | Butt U, Charalambous CP. Complications associated with open coracoid transfer procedures for shoulder instability. J Shoulder Elbow Surg 2012;21:1110-9.
|
| 9. | Meyer DC, Moor BK, Gerber C, Ek ET. Accurate coracoid graft placement through use of a drill guide for the Latarjet procedure. J Shoulder Elbow Surg 2013;22:701-8.
|
| 10. | Shah AA, Butler RB, Romanowski J, Goel D, Karadagli D, Warner JJ. Short-term complications of the Latarjet procedure. J Bone Joint Surg Am 2012;94:495-501.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
| This article has been cited by | | 1 |
Arthroscopic Bone Graft Procedure for Anterior Inferior Glenohumeral Instability |
|
| Ettore Taverna,Riccardo DæAmbrosi,Carlo Perfetti,Guido Garavaglia | | Arthroscopy Techniques. 2014; | | [Pubmed] | [DOI] | |
|
|
|
|














