| |


 |
| Year : 2015 | Volume
: 9
| Issue : 2 | Page : 38-42 |
|
|
|
|
|
ORIGINAL ARTICLE Scapular neck length and implications for reverse total shoulder arthroplasty: An anatomic study of 442 cadaveric specimens
Chad M Fortun1, Jonathan J Streit1, Steven A Horton1, Stephanie J Muh2, Robert J Gillespie1, Reuben Gobezie1
1 The Cleveland Shoulder Institute, Department of Orthopaedics, University Hospitals of Cleveland, Cleveland, OH 44024, USA
2 Department of Orthopedics, Henry Ford Hospital, Detroit, MI 48202, USA
Correspondence Address:
Reuben Gobezie
UH Ahuja Medical Center, 3999 Richmond Road, Beachwood, OH 44122
USA
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.154754
 |
|
|
|
| Date of Web Publication | 8-Apr-2015 |
 Abstract Abstract | | |
Purpose: Reverse total shoulder arthroplasty (RTSA) may be used to treat a variety of pathologic shoulder conditions, but complications such as scapular notching continue raise concerns. Variable anatomy surrounding the glenoid may have implications for future RTSA design, but at present the anatomy of the scapular neck in the human population has not been clearly defined.
Materials and Methods: 442 human scapulae from the Hamann-Todd Osteological Collection were measured for scapular neck length (SNL) and scapular neck angle (SNA). SNL was defined as the distance from the most lateral portion of the infraglenoid tubercle to the most inferolateral portion of the glenoid fossa. The SNA was measured according to Gerber et al. previously. The mean, standard deviation and ranges for SNL and SNA were calculated and compared based on sex and race, and interobserver variability was calculated.
Results: The mean SNL was 1.06 cm ± 0.33 cm (0.37-2.43 cm). Males demonstrated a larger SNL (1.08 cm ± 0.33 cm) than females (1.01 cm ± 0.32 cm) (P < 0.12), and Caucasians (1.09 cm ± 0.33 cm) demonstrated a significantly larger SNL than African-Americans (1.00 cm ± 0.32) (P < 0.01). The mean SNA was 106.7° ± 11.0° (76.9-139.4°). No significant correlation was found between SNL and SNA (Pearson Correlation Coefficient = 0.018) (P < 0.702).
Conclusion: Scapular neck length and SNA vary widely within the population but there appears to be a tendency towards increased SNL in males and Caucasians.
Clinical Relevance: The anatomy of the scapular neck may have significant implications for RTSA design, surgical planning, and reduction of associated complications.
Keywords: Notching, reverse total shoulder arthroplasty, scapular neck angle, scapular neck length
How to cite this article:
Fortun CM, Streit JJ, Horton SA, Muh SJ, Gillespie RJ, Gobezie R. Scapular neck length and implications for reverse total shoulder arthroplasty: An anatomic study of 442 cadaveric specimens. Int J Shoulder Surg 2015;9:38-42 |
How to cite this URL:
Fortun CM, Streit JJ, Horton SA, Muh SJ, Gillespie RJ, Gobezie R. Scapular neck length and implications for reverse total shoulder arthroplasty: An anatomic study of 442 cadaveric specimens. Int J Shoulder Surg [serial online] 2015 [cited 2016 Sep 20];9:38-42. Available from: http://www.internationalshoulderjournal.org/text.asp?2015/9/2/38/154754 |
| Introduction | |  |
Reverse total shoulder arthroplasty (RTSA) is a popular treatment for rotator cuff tear arthropathy and other painful shoulder conditions in which the rotator cuff is deficient. Scapular notching is an important complication that occurs in up to 96% of patients [1],[2],[3] and has been correlated with poorer clinical outcomes, chronic inflammation, osteolysis, and early prosthesis failure. [2],[4] The exact cause of scapular notching and methods for preventing this complication are poorly understood. Recently, investigative work has focused on delineating the various implant related factors influencing the incidence of scapular notching. [1],[5],[6],[7] Earlier studies have demonstrated anatomical variations in the anatomy of patient scapulae and the influence that patient anatomy has on the development of scapular notching. [4],[8] These studies have demonstrated that there is no one-size-fits-all approach to RTSA that will provide an optimal impingement free range of motion. [1],[4],[8] Scapular neck length (SNL) or the lateral offset of the humerus from the glenoid, has been shown to have a large influence over the rate of scapular notching. [5],[6] Frankle et al. have shown in numerous studies, both clinically and in the laboratory that lateralization of the humerus dramatically reduces the rate of scapular notching. [6],[9] Recently, Paisley et al. have demonstrated significant variability in SNL in a small series of patients. [10] However, there are currently no studies that have characterized the variations in SNL in a large body of human specimens.
The purpose of this study is to characterize the SNL in a large body of patient scapulae using the Haman-Todd Osteological Collection, one of the largest osteological collections of complete human skeletons in the world. We hypothesize that the ability to understand the variations in SNL across a population of patients will enable us to minimize scapular notching by incorporating SNL measurements into the reconstruction plan of patients undergoing RTSA's. Our secondary hypothesis is that measurements of the SNL and scapular neck angle (SNA), using defined anatomic landmarks, would be reproducible between investigators, and that these measurements would differ considerably between individuals.
| Materials and methods | | |
For the purposes of this study, we obtained 442 dry human scapulae from the Hamann-Todd Osteological Collection, which is housed in the Cleveland Museum of Natural History (Cleveland, OH). This collection contains over 3000 complete disarticulated human skeletons that were preserved and prepared by Case Western Reserve University School of Medicine faculty from unclaimed remains at the Cleveland city morgue between 1912 and 1938. Scapulae were randomly chosen from the collection. Inclusion criteria included adult human skeletons, age 18-65, with intact bilateral scapulae. Exclusion criteria included pediatric skeletons, those with damaged or missing scapulae and those skeletons without a bilateral set. Digital photographs of scapulae using a standardized posteroanterior view were obtained, which was chosen based on work by Handling et al. [11] who described the insertion of the long head of the triceps on the posterior lateral portion of the scapula at the infraglenoid tubercle. For the purposes of photography and measurement, the scapula was positioned at a standard distance from the camera lense. Specifically the scapula was positioned along the craniocaudal axis to allow the glenoid fossa anterior and posterior margins to be flush and parallel to the camera. The scapula was positioned along the medial-to-lateral axis so that the entire glenoid fossa could be visualized free of obstruction from the acromion. SNL was defined as the distance from the most lateral portion of the infraglenoid tubercle to the most inferolateral portion of the glenoid fossa [Figure 1]. The infraglenoid tubercle was consistently found in a location that could be alternatively located by following the topographical change at the neck-body junction that coursed inferiorly from the spinoglenoid notch to the most lateral extent of the infraglenoid tubercle [Figure 2]. This was used as an additional criterion for location of the tubercle if its location was not immediately obvious. The SNA, as defined by Simovitch et al., [4] was measured as the intersection of a line parallel to the face of the glenoid and a second line between the inferior glenoid rim and a point 1 cm along the inferior border of the scapula. | Figure 1: Novel measurement of scapular neck length indicated by yellow line. Length determined from lateral edge of infraglenoid tubercle to lateral edge of inferior glenoid
Click here to view |
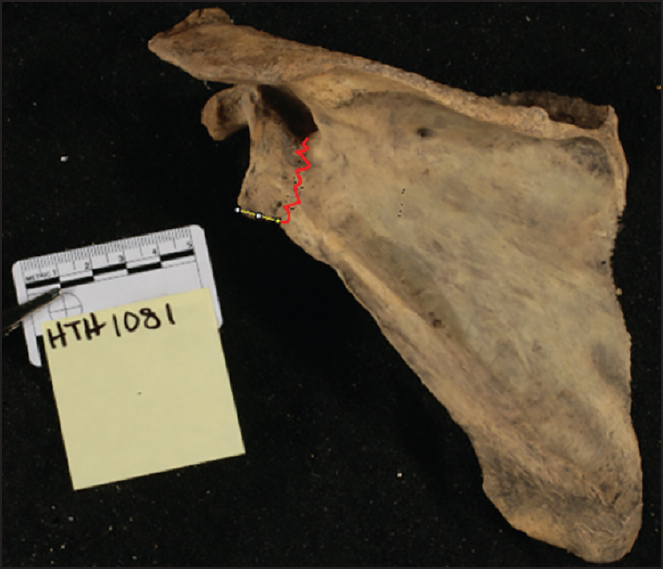 | Figure 2: Measurement of scapular neck length assisted by topographical change noted from spinoglenoid notch to lateral border of infraglendoid tubercle as indicated by red line
Click here to view |
The mean, standard deviation, and ranges for SNL and SNA were calculated and compared between groups based on sex and race using a Student's t-test. A single examiner performed all digital measurements using standard ImageJ NIH type software. Interobserver and intraobserver reliability for scapular neck measurements were performed by four of the authors in order to determine the validity of our measurement protocol using the intraclass correlation coefficient. Significance for all statistical tests was set at P < 0.05.
| Results | | |
Our study population consisted of 221 cadaveric specimens (188 male, 33 female) of mean age 45.1 years at the time of death. 165 specimens were Caucasian, and 56 were African-American [Table 1]. The scapular neck could be measured bilaterally in all specimens, for a total of 442 scapulae measured. The mean SNL for our study cohort was 10.6 mm ± 3.3 mm (range 3.7-24.3 mm). The mean SNL for the left scapula was 10.4 mm ± 3.4 mm, and the mean SNL for the right scapula was 10.7 mm ± 3.5 mm (P < 0.36). Males had a slightly larger SNL (10.8 mm ± 3.3 mm) than females (10.1 mm ± 3.2 mm), which was not statistically significant (P < 0.12). Caucasians had a larger SNL (10.9 mm ± 3.3 mm) than African-Americans (10.0 mm ± 0.32) that was statistically significant (P < 0.01). Intra-observer reliability for the measurement of SNL was 0.973, and inter-observer reliability was 0.856 (95% confidence interval [CI] = 0.716-0.937).
The mean SNA was 106.7° ± 11.0°, and ranged from 76.9° to 139.4°. The mean SNA for the left scapula was 107.1° ± 10.3°, and the mean SNA for the right scapula was 106.3° ± 11.5° (P < 0.29). Males demonstrated a mean SNA of 106.5° ± 10.7°, and the mean SNA for females was 107.3° ± 12.6° (P < 0.59). The mean SNA for Caucasians was 107.2° ± 11.1°, and the mean for African-Americans was 105.3° ± 10.7° (P < 0.10). Interobserver reliability for the measurement of SNA was 0.682 (95% CI = 0.348-0.861), and the intraobserver reliability was 0.681 (95% CI = 0.363-0.859). No significant correlation was found between SNL and SNA (Pearson Correlation Coefficient = 0.018) (P = 0.702) [Figure 3].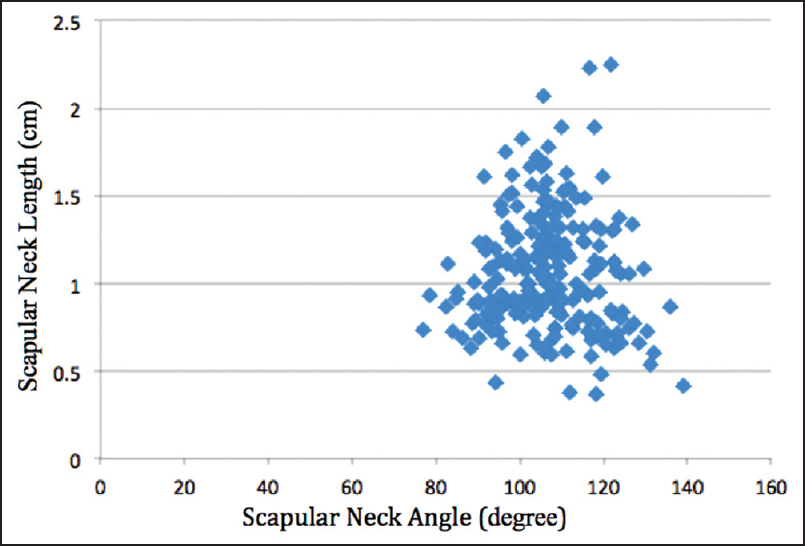 | Figure 3: No significant correlation between scapular neck angle (deg, X-axis) and scapular neck length (cm, Y-axis)
Click here to view |
| Discussion | | |
We have performed the largest anatomic study of scapular neck morphology using 442 dry cadaveric specimens from an osteological collection, and we report the mean and ranges for the SNL and SNA with respect to sex and race. Our hypothesis that these measurements would be reproducible between investigators was confirmed, as was our hypothesis that significant differences in SNL and SNA would be identified. The relationship between race and sex demonstrated that the SNL was insignificantly larger in males and significantly larger in the Caucasian population. However, the absolute value of these race and sex differences were quite small, making this finding difficult to interpret, and creating a need for the future follow up studies.
The anatomy of the scapula has long been of interest to shoulder surgeons, but few anatomic studies have been performed in order to identify differences within the population that may impact the treatment of shoulder pathology. Multiple studies have discussed the wide variation in glenoid morphology, [6],[12],[13],[14],[15] especially as this relates to traumatic and degenerative disease. However, although SNL and SNA have both been implicated as contributing to complications and functional outcomes after reverse shoulder arthroplasty, [2],[4],[16] ours is the first study to define the population means and ranges for these parameters. Torrens et al. [17] previously measured the SNL of cadaveric specimens using a reference from the most inferolateral edge of the glenoid fossa to the most lateral extent of the posterior column to define the SNL. However, our analysis of the scapula demonstrated significant variability in determining the lateral extent of the posterior column. Our study instead demonstrated a consistent finding of the infraglenoid tubercle from the posterior view, and we propose this functional SNL should be defined as the portion of the lateral border of the scapula from the most lateral edge of the infraglenoid tubercle to the most inferolateral edge of the glenoid fossa [Figure 1]. As stated by Middernacht et al., the majority of scapular notching occurs in the first cm of the scapular neck [8] which appears to be related to the position of the infraglenoid tubercle. A far lateral infraglenoid tubercle implies a shorter functional SNL and an increased propensity for scapular notching.
Our study has established population norms for SNL and SNA using a large sample size, and based on the wide variation in these parameters, greater customization in RTSA design may be necessary. We found SNL to be highly variable among specimens, with a minimum of 3.7 mm and a maximum of 24.3 mm, which represents more than a 6-fold difference in SNL within our population [Figure 4]. The variability of SNA within our population was also high, with a large range of 76.9-139.4°. In the setting of RTSA, previous studies have postulated that acute angles, or superior tilting of the glenosphere, can lead to increased scapular notching and early prosthesis failure while large angles, or inferior tilting of the glenosphere may be protective against scapular notching. [4],[7],[18],[19] One can propose that patients with a short SNL, an acute SNA or a combination there of may be prone to scapular notching. It can also be hypothesized that using a lateralized RTSA design in a patient with a long scapular neck may excessively lateralize the scapulohumeral articulation, leading to increased risk of acromial stress fracture. Comparatively, for patients with a short SNL, others have lateralized the center of rotation using bone graft or a lateralized RTSA design, [5],[9],[20] which may lead to greater external rotation, improved deltoid contour, and diminished notching. [21] It is likely that the SNL and the SNA plays a large role in scapular notching, and should be taken into account when planning for RTSA. Greater customization of RTSA implants would help surgeons better fit patients based on their native anatomy, which may improve clinical outcomes and reduce complications.
Limitations of the present study relate to its design using cadaveric specimens, which limits the conclusions that may be drawn regarding the function of these shoulders in daily life. It is unknown whether any of these persons may have had shoulder pain or other issues related to their anatomy. In addition, our study population contained only African-American and Caucasian specimens, which limits the conclusions that may be drawn regarding other ethnicities. Future studies may analyze the impact of SNL and SNA on scapular notching, range of motion, and functional outcomes using different implant designs, as well as develop optimal imaging techniques to better assess preoperative scapular anatomy for use in surgical planning.
| Conclusion | | |
A wide range of SNL s and SNAs were observed in our study population, and only small differences were noted based on sex and race. The anatomy of the scapular neck may have significant implications for RTSA design and surgical planning, and greater attention to matching a patient's native anatomy may ultimately reduce the incidence of complications such as scapular notching.
| References | | |
| 1. | Gerber C, Pennington SD, Nyffeler RW. Reverse total shoulder arthroplasty. J Am Acad Orthop Surg 2009;17:284-95.  |
| 2. | Nicholson GP, Strauss EJ, Sherman SL. Scapular notching: Recognition and strategies to minimize clinical impact. Clin Orthop Relat Res 2011;469:2521-30. |
| 3. | Roche C, Flurin PH, Wright T, Crosby LA, Mauldin M, Zuckerman JD. An evaluation of the relationships between reverse shoulder design parameters and range of motion, impingement, and stability. J Shoulder Elbow Surg 2009;18:734-41. |
| 4. | Simovitch RW, Zumstein MA, Lohri E, Helmy N, Gerber C. Predictors of scapular notching in patients managed with the Delta III reverse total shoulder replacement. J Bone Joint Surg Am 2007;89:588-600. |
| 5. | Boileau P, Moineau G, Roussanne Y, O′Shea K. Bony increased-offset reversed shoulder arthroplasty: Minimizing scapular impingement while maximizing glenoid fixation. Clin Orthop Relat Res 2011;469:2558-67. |
| 6. | Frankle MA, Teramoto A, Luo ZP, Levy JC, Pupello D. Glenoid morphology in reverse shoulder arthroplasty: Classification and surgical implications. J Shoulder Elbow Surg 2009;18:874-85. |
| 7. | Gutiérrez S, Comiskey CA th, Luo ZP, Pupello DR, Frankle MA. Range of impingement-free abduction and adduction deficit after reverse shoulder arthroplasty. Hierarchy of surgical and implant-design-related factors. J Bone Joint Surg Am 2008;90:2606-15. |
| 8. | Middernacht B, De Roo PJ, Van Maele G, De Wilde LF. Consequences of scapular anatomy for reversed total shoulder arthroplasty. Clin Orthop Relat Res 2008;466:1410-8. |
| 9. | Frankle M, Levy JC, Pupello D, Siegal S, Saleem A, Mighell M, et al. The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency. A minimum two-year follow-up study of sixty patients surgical technique. J Bone Joint Surg Am 2006;88 Suppl 1 Pt 2:178-90. |
| 10. | Paisley KC, Kraeutler MJ, Lazarus MD, Ramsey ML, Williams GR, Smith MJ. Relationship of scapular neck length to scapular notching after reverse total shoulder arthroplasty by use of plain radiographs. J Shoulder Elbow Surg 2014;23:882-7. |
| 11. | Handling MA, Curtis AS, Miller SL. The origin of the long head of the triceps: A cadaveric study. J Shoulder Elbow Surg 2010;19:69-72. |
| 12. | Kwon YW, Powell KA, Yum JK, Brems JJ, Iannotti JP. Use of three-dimensional computed tomography for the analysis of the glenoid anatomy. J Shoulder Elbow Surg 2005;14:85-90. |
| 13. | Scalise JJ, Bryan J, Polster J, Brems JJ, Iannotti JP. Quantitative analysis of glenoid bone loss in osteoarthritis using three-dimensional computed tomography scans. J Shoulder Elbow Surg 2008;17:328-35. |
| 14. | Walch G, Badet R, Boulahia A, Khoury A. Morphologic study of the glenoid in primary glenohumeral osteoarthritis. J Arthroplasty 1999;14:756-60. |
| 15. | Walch G, Boulahia A, Boileau P, Kempf JF. Primary glenohumeral osteoarthritis: Clinical and radiographic classification. The Aequalis Group. Acta Orthop Belg 1998;64 Suppl 2:46-52. |
| 16. | Cheung E, Willis M, Walker M, Clark R, Frankle MA. Complications in reverse total shoulder arthroplasty. J Am Acad Orthop Surg 2011;19:439-49. |
| 17. | Torrens C, Corrales M, Gonzalez G, Solano A, Cáceres E. Cadaveric and three-dimensional computed tomography study of the morphology of the scapula with reference to reversed shoulder prosthesis. J Orthop Surg Res 2008;3:49. |
| 18. | Nyffeler RW, Werner CM, Simmen BR, Gerber C. Analysis of a retrieved delta III total shoulder prosthesis. J Bone Joint Surg Br 2004;86:1187-91. |
| 19. | Sirveaux F, Favard L, Oudet D, Huquet D, Walch G, Molé D. Grammont inverted total shoulder arthroplasty in the treatment of glenohumeral osteoarthritis with massive rupture of the cuff. Results of a multicentre study of 80 shoulders. J Bone Joint Surg Br 2004;86:388-95. |
| 20. | Kempton LB, Balasubramaniam M, Ankerson E, Wiater JM. A radiographic analysis of the effects of prosthesis design on scapular notching following reverse total shoulder arthroplasty. J Shoulder Elbow Surg 2011;20:571-6. |
| 21. | Valenti P, Sauziéres P, Cogswell L, O′Toole G, Katz D. The reverse shoulder prosthesis - surgical technique. Tech Hand Up Extrem Surg 2008;12:46-55. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
[Table 1]
|














