| |


 |
| Year : 2015 | Volume
: 9
| Issue : 2 | Page : 43-46 |
|
|
|
|
|
ORIGINAL ARTICLE The accuracy of "subacromial grind test" in diagnosis of supraspinatus rotator cuff tears
Seif Sawalha1, Jochen Fischer2
1 Specialist Trainee (ST6) Trauma and Orthopaedics, Mersey Deanery, Liverpool, Macclesfield, United Kingdom
2 Macclesfield District General Hospital, Department of Orthopaedics, Macclesfield, United Kingdom
Correspondence Address:
Seif Sawalha
Flat 158, Waterloo Warehouse, Liverpool, L3 0BH
United Kingdom
 Source of Support: None, Conflict of Interest: None
Read associated with this article DOI: 10.4103/0973-6042.154756
 |
|
|
|
| Date of Web Publication | 8-Apr-2015 |
 Abstract Abstract | | |
Purpose: The aim of this study is to assess the accuracy of a simple clinical test (subacromial grind test) in diagnosing supraspinatus tendon tears.
Patients and Methods: The test is considered positive if palpable crepitus or grinding is detected on passive internal and external rotation of the shoulder while abducted in the scapular plane. Data were collected prospectively on 47 patients undergoing shoulder arthroscopy, and the results of the test and arthroscopy compared.
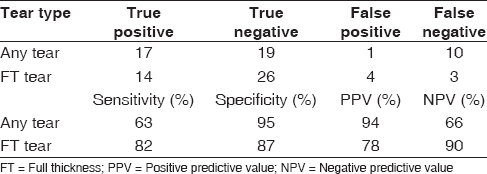
Results: During arthroscopy, 17 patients had full thickness (FT) tears of supraspinatus tendon and 10 had partial thickness tears. For any supraspinatus tear, the sensitivity of the test was 63%, specificity 95%, positive predictive value 94%, negative predictive value 66% and overall accuracy 79%. For FT tears, the sensitivity was 82%, specificity 87%, positive predictive value 78%, negative predictive value 90% and overall accuracy 85%.
Conclusion: We found that this is a useful single test for diagnosing FT supraspinatus tears.
Level of Evidence: Level IV diagnostic study.
Keywords: Grind, physical examination, shoulder, supraspinatus tendon, tear
How to cite this article:
Sawalha S, Fischer J. The accuracy of "subacromial grind test" in diagnosis of supraspinatus rotator cuff tears. Int J Shoulder Surg 2015;9:43-6 |
| Introduction | |  |
Rotator cuff pathology is a common problem with rising incidence and increasing volume of surgical repair. [1] Despite advances in imaging modalities, the role of physical examination in diagnosing rotator cuff tears remains important. Degenerative cuff tears commonly start in supraspinatus tendon. Many physical examination tests have been described for diagnosing supraspinatus tears. Frequently used tests include empty can test (Jobe test), full can test and drop arm test. The diagnostic accuracy of these tests in the literature is highly variable. [2],[3]
Codman described direct palpation of rotator cuff tears in 1934. He also described "soft crepitus" palpable with the "tip of finger pressing on sulcus and eminence" as one of the signs of complete rupture of supraspinatus tendon. [4] The accuracy of trans-deltoid palpation of the defect in the tendon described by Codman (rent test) in the diagnosis of rotator cuff tears has been assessed. [5],[6] However, the usefulness of palpable crepitus in diagnosis of rotator cuff tears has not been studied.
The aim of the study is to assess the accuracy of the subacromial grind test in diagnosing supraspinatus tendon tears using shoulder arthroscopy as reference.
| Patients and methods | | |
Previous papers that studied similar patient population to ours reported approximately 42% prevalence of full thickness (FT) rotator cuff tears at arthroscopy. [6] We anticipated a 90% specificity of the test with 0.1 precision and 95% confidence level (i.e., specificity between 80% and 100%). Using a simple nomogram designed for sample size calculation in diagnostic studies, the required number of subjects is approximately 50. [7]
We prospectively collected data on 50 consecutive patients who underwent shoulder arthroscopy between February and August 2013. We included 47 patients (31 male and 16 female, mean age 58 years (range 27-76 years). Three patients could not tolerate the test due to pain and therefore, were excluded. All patients presented with a shoulder complaint and had already been fully assessed in shoulder clinics. The patients were assessed on the day of their operations, several weeks after their clinic appointments, by the authors. At the time of performing the subacromial grind test, the authors were blinded to patients' clinical and radiological findings in clinics and the proposed arthroscopic procedures. The result of the subacromial grind test recorded as positive or negative. The intraoperative findings (presence of supraspinatus tendon tear and the degree of tear; FT or partial thickness [PT]) were recorded.
Statistical analysis
A 2 × 2 table was designed, and sensitivity, specificity, positive and negative predictive values were calculated. Receiver operating characteristic (ROC) curve analysis was performed using SPSS version 20 statistics software (IBM, Armonk, NY, USA) and the area under the curve (AUC) value calculated. A P < 0.05 was considered as statistically significant.
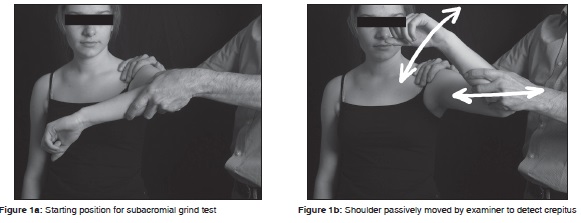
The subacromial grind test description
With the patient standing and examiner standing facing the patient, the examiner grasps the patient's flexed elbow. The shoulder is passively abducted in the scapular plane to 90° (Hawkins-Kennedy test position). [8] The examiner's other hand is placed over the patient's shoulder overlying the anterior acromion and greater tuberosity. The examiner passively internally and externally rotates the shoulder detecting the presence of palpable crepitus [Figure 1]a and b. The test was considered positive if resulted in palpable crepitus.
The anatomic basis for Hawkins-Kennedy test position was studied previously. Pappas et al. demonstrated subacromial narrowing and contact with suprasinatus in most cases during open magnetic resonance imaging (MRI). [9] Roberts et al. showed using MRI scans that the rotator cuff insertion appeared to be in closest proximity to the anteroinferior acromion at 90° of flexion. [10]
| Results | | |
[Table 1] summarizes the findings of the test and arthroscopy, and sensitivity analysis. During arthroscopy, 17 patients had FT tears of supraspinatus tendon, and 10 had PT tears. Three patients had false negative tests; two of them had massive cuff tears involving all tendons. Four patients had false positive tests; three of them had PT tears (two bursal side tears and one joint surface tear), and one had no tears. None of the patients had other pathologies.
Results of sensitivity and specificity analysis are shown in [Table 1]. The test was more sensitive for detection of FT tears. ROC curve analysis showed that for FT tears AUC = 0.85 (95% confidence interval [CI] 0.72-0.97) (P < 0.0005) indicating a good test while for any tear, the AUC = 0.79 (95% CI 0.66-0.92) (P = 0.001) indicating a fair test.
| Discussion | | |
The study shows that the subacromial grind test has a very good accuracy and differentiates well between patients with and without FT tears. The test was well-tolerated by most patients. We found the subacromial grind test to be simple and could be easily incorporated into the shoulder physical examination sequence. It relies on an objective sign (crepitus) and therefore, is not affected by patient factors like poor effort and secondary gain. We assessed the test's accuracy against shoulder arthroscopy as the gold standard for diagnosis. The results show that it is mostly useful for detecting FT supraspinatus tears.
Several papers and systematic reviews have investigated the usefulness of clinical examination tests for diagnosis of rotator cuff tears. While external rotation lag sign is a very sensitive and specific test for diagnosis of infraspinatus and teres minor tears, the tests for detecting supraspinatus tears are less useful. [2],[3] The sensitivities and specificities of empty can test (Jobe test) and full can test in the literature is very variable. [11],[12],[13] Several factors could explain this wide variability; the grade of cuff tears, how the test is performed (pain, weakness or both), the reference gold standard (arthroscopy, MRI or ultrasound) and the patient population being studied.
Compared to the subacromial grind test, the Jobe test (with weakness as a response) has 52% sensitivity and 82% specificity for FT tears. [14] When the Jobe test was compared against MRI scans, sensitivities ranging from 60% to 77% and specificities from 68% to 89% were reported. Considering the pain and/or weakness as a response improves the sensitivity of the test but the specificity drops. The full can test has a largely similar accuracy to the Jobe test. [12],[13] The Codman's drop arm sign has a higher reported specificity than the subacromial grind test, but its sensitivity is much lower. [14],[15]
Impingement tests, like Neer's and Hawkins-Kennedy signs, were also assessed for their usefulness in detecting cuff tears, but their diagnostic accuracy were low. [11],[14],[16] A recently described test, the lateral Jobe test, is reported to have high sensitivity and specificity, but it has not been independently assessed and is not widely used. [17]
Two previous studies assessed trans-deltoid palpation of rotator cuff tears (rent test). Lyons and Tomlinson reported 91% sensitivity and 75% specificity, but they also assessed supraspinatus and infraspinatus muscle strengths and not the rent test in isolation. [5] Wolf and Agrawal reported a diagnostic accuracy of 96.3% for rent test. The rent test involves direct palpation of the defect in the cuff tendon, which requires experience and could be painful and difficult especially in obese patients with thick fatty layer over the shoulder. [6]
Our study has limitations. First, our group of patients was preselected for arthroscopy. We do not know if the same sensitivity and specificity will be reproduced in a different group of patients. Every possible measure was taken to avoid bias by blinding the assessors to patients' clinical and radiologic records in addition to the long-time interval between clinic and operation dates. The study population included patients with different shoulder problems in addition to impingement and cuff tears (e.g., instability, superior labral anterior-posterior tears, acromioclavicular joint osteoarthritis) and therefore, we think it is representative of a shoulder clinic patient population. Second, inter-or intra-observer reliability of the new test is not available as the study included a single assessor. Third, the study is possibly underpowered as three patients who could not tolerate the test were excluded. The subacromial grind test had good but not excellent accuracy in our study (85%). Some studies suggested that other structures also impinge in the Hawkins-Kennedy test position, which could explain why the test did not have higher sensitivity and specificity. [18],[19]
There are other shoulder pathologies, not found in our study population that are associated with crepitus and could result in a false positive test. Advanced glenohumeral arthritis is associated with coarse bony crepitus. Scapulothoracic disorders like bursitis or osteochondroma often present with crepitus but this is usually audible and reproduced by active rather than passive movement. [20]
Despite the limitations, we conclude that the subacromial grind test is useful as a single test for diagnosis of FT supraspinatus tears. It is simple and easy to perform, requires minimal effort by the patient and can be easily included in the physical examination sequence.
| References | | |
| 1. | White JJ, Titchener AG, Fakis A, Tambe AA, Hubbard RB, Clark DI. An epidemiological study of rotator cuff pathology using The Health Improvement Network database. Bone Joint J 2014;96:350-3.  |
| 2. | Hanchard NC, Lenza M, Handoll HH, Takwoingi Y. Physical tests for shoulder impingements and local lesions of bursa, tendon or labrum that may accompany impingement. Cochrane Database Syst Rev 2013;4:CD007427. |
| 3. | Hegedus EJ, Goode AP, Cook CE, Michener L, Myer CA, Myer DM, et al. Which physical examination tests provide clinicians with the most value when examining the shoulder? Update of a systematic review with meta-analysis of individual tests. Br J Sports Med 2012;46:964-78. |
| 4. | |
| 5. | Lyons AR, Tomlinson JE. Clinical diagnosis of tears of the rotator cuff. J Bone Joint Surg Br 1992;74:414-5. |
| 6. | Wolf EM, Agrawal V. Transdeltoid palpation (the rent test) in the diagnosis of rotator cuff tears. J Shoulder Elbow Surg 2001;10:470-3. |
| 7. | Malhotra RK, Indrayan A. A simple nomogram for sample size for estimating sensitivity and specificity of medical tests. Indian J Ophthalmol 2010;58:519-22. [ PUBMED]  |
| 8. | Hawkins RJ, Kennedy JC. Impingement syndrome in athletes. Am J Sports Med 1980;8:151-8. [ PUBMED] |
| 9. | Pappas GP, Blemker SS, Beaulieu CF, McAdams TR, Whalen ST, Gold GE. In vivo anatomy of the Neer and Hawkins sign positions for shoulder impingement. J Shoulder Elbow Surg 2006;15:40-9. |
| 10. | Roberts CS, Davila JN, Hushek SG, Tillett ED, Corrigan TM. Magnetic resonance imaging analysis of the subacromial space in the impingement sign positions. J Shoulder Elbow Surg 2002;11:595-9. |
| 11. | Bak K, Sørensen AK, Jørgensen U, Nygaard M, Krarup AL, Thune C, et al. The value of clinical tests in acute full-thickness tears of the supraspinatus tendon: Does a subacromial lidocaine injection help in the clinical diagnosis? A prospective study. Arthroscopy 2010;26:734-42. |
| 12. | Itoi E, Kido T, Sano A, Urayama M, Sato K. Which is more useful, the "full can test" or the "empty can test," in detecting the torn supraspinatus tendon? Am J Sports Med 1999;27:65-8. |
| 13. | Kim E, Jeong HJ, Lee KW, Song JS. Interpreting positive signs of the supraspinatus test in screening for torn rotator cuff. Acta Med Okayama 2006;60:223-8. |
| 14. | Park HB, Yokota A, Gill HS, El Rassi G, McFarland EG. Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. J Bone Joint Surg Am 2005;87:1446-55. |
| 15. | Murrell GA, Walton JR. Diagnosis of rotator cuff tears. Lancet 2001;357:769-70. [ PUBMED] |
| 16. | MacDonald PB, Clark P, Sutherland K. An analysis of the diagnostic accuracy of the Hawkins and Neer subacromial impingement signs. J Shoulder Elbow Surg 2000;9:299-301. |
| 17. | Gillooly JJ, Chidambaram R, Mok D. The lateral Jobe test: A more reliable method of diagnosing rotator cuff tears. Int J Shoulder Surg 2010;4:41-3. [ PUBMED] |
| 18. | Tucker S, Taylor NF, Green RA. Anatomical validity of the Hawkins-Kennedy test - a pilot study. Man Ther 2011;16:399-402. |
| 19. | Valadie AL 3 rd , Jobe CM, Pink MM, Ekman EF, Jobe FW. Anatomy of provocative tests for impingement syndrome of the shoulder. J Shoulder Elbow Surg 2000;9:36-46. |
| 20. | Rockwood CA Jr, Matsen FA 3 rd , Wirth MA, Lippitt SB. Clinical Evaluation of Shoulder Problems. In: The Shoulder. 4 th ed., Ch. 4. Published by Elsevier; 2009. Available from: https://www.inkling.com/read/rockwood-matsen-shoulder-4th/chapter-4/special-tests. [Last cited on 2014 Oct 04]. |
[Figure 1]
[Table 1]
|