| |


 |
| Year : 2015 | Volume
: 9
| Issue : 2 | Page : 56-59 |
|
|
|
|
|
SURGICAL TECHNIQUE An innovative method of fracture reduction in an arthroscopically assisted cannulated screw fixation of an Ideberg type III glenoid fracture
Sandra J Bonczek, Richard Hutchinson, Jagannath Chakravarthy
Department of Trauma and Orthopedics, Queen Elizabeth Hospital, Sheriff Hill, Gateshead NE9 6SX, United Kingdom
Correspondence Address:
Richard Hutchinson
Department of Trauma and Orthopedics, Queen Elizabeth Hospital, Sheriff Hill, Gateshead NE9 6SX
United Kingdom
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.154770
 |
|
|
|
| Date of Web Publication | 8-Apr-2015 |
 Abstract Abstract | | |
Significantly displaced intra-articular glenoid fractures treated nonoperatively have been found to have poor functional outcomes. For this reason, most are treated with open reduction and internal fixation. Conventional open techniques involve extensive exposure and soft tissue dissection. Moreover, visualization of the fracture and its reduction can also be difficult even with standard open techniques. We present a case of an Ideberg type III glenoid fracture treated with an arthroscopically assisted percutaneous screw fixation, using the coracoid as a reduction aide. This reduction technique is not previously reported in the literature. Arthroscopically assisted percutaneous glenoid fixation has showed promising early results in the literature. In our case, the fracture united and the patient returned to all his normal daily activities by 7 weeks postoperatively. This suggests arthroscopically assisted glenoid fixation provides good functional and radiological outcomes, without the need for extensive soft tissue dissection.
Keywords: Arthroscopic, fracture, glenoid, percutaneous, reduction
How to cite this article:
Bonczek SJ, Hutchinson R, Chakravarthy J. An innovative method of fracture reduction in an arthroscopically assisted cannulated screw fixation of an Ideberg type III glenoid fracture. Int J Shoulder Surg 2015;9:56-9 |
How to cite this URL:
Bonczek SJ, Hutchinson R, Chakravarthy J. An innovative method of fracture reduction in an arthroscopically assisted cannulated screw fixation of an Ideberg type III glenoid fracture. Int J Shoulder Surg [serial online] 2015 [cited 2016 Sep 20];9:56-9. Available from: http://www.internationalshoulderjournal.org/text.asp?2015/9/2/56/154770 |
| Introduction | |  |
Scapular fractures account for just 0.7% of all fractures. [1] Of these, only 10% are intra-articular, and 1% have significant displacement. [2] However, treated conservatively displaced intra-articular glenoid fractures have been found to have poor functional outcomes and thus, most are now treated with open reduction and internal fixation as this allows accurate reduction of the articular surface under direct vision. More recently, minimally invasive techniques using arthroscopy to visualize the reduction of the articular surface have been described with good results. [3],[4],[5] Here, we describe the case of an Ideberg type III fracture treated with a minimally invasive arthroscopic surgical technique in which the coracoid process is used as a reduction tool.
| Case report | | |
In our case, a 70-year-old male sustained a right glenoid fracture after falling 8 feet from a ladder. X-rays of the shoulder showed a complex intra-articular scapula fracture [Figure 1]. A computed tomography (CT) scan was done which identified a comminuted fracture of the glenoid with superior-medial extension through the scapula spine, in fitting with an Ideberg type III injury. It also showed a 5 mm intra-articular step in the glenoid on the coronal views, with superior subluxation of the humeral head [Figure 2]. | Figure 1: Anteroposterior radiograph of the right shoulder showing a displaced Ideberg type III fracture of the gleniod, with some ipsilateral rib fractures
Click here to view |
 | Figure 2: Coronal computed tomography scan image of the right shoulder revealing a 5 mm intra-articular step in the gleniod surface
Click here to view |
The fracture was treated with an arthroscopically assisted cannulated screw fixation, using the coracoid as a reduction tool, 5 days postinjury.
| Surgical technique | | |
The surgery was performed under general anesthesia with an interscalene nerve block. The patient was placed in a semi-reclined "beach chair" position. The arm was draped free without any traction.
Preliminary radiographs were taken prior to draping to confirm adequate visualization of the glenoid. A posterior portal was used as a viewing portal. The hematoma was evacuated with saline lavage and the fracture identified. An additional anterior working portal was used to evaluate the intra-articular structures. No cannulae were used. The large articular step was visualized, and mobility of the fracture was confirmed with an arthroscopy hook [Figure 3]. The rotator cuff and biceps were visualized. The biceps tendon was frayed and, therefore, a biceps tenotomy was performed. This highlights the advantage of identifying and potentially treating concurrent intra-articular glenohumeral joint pathology when using an arthroscopic technique.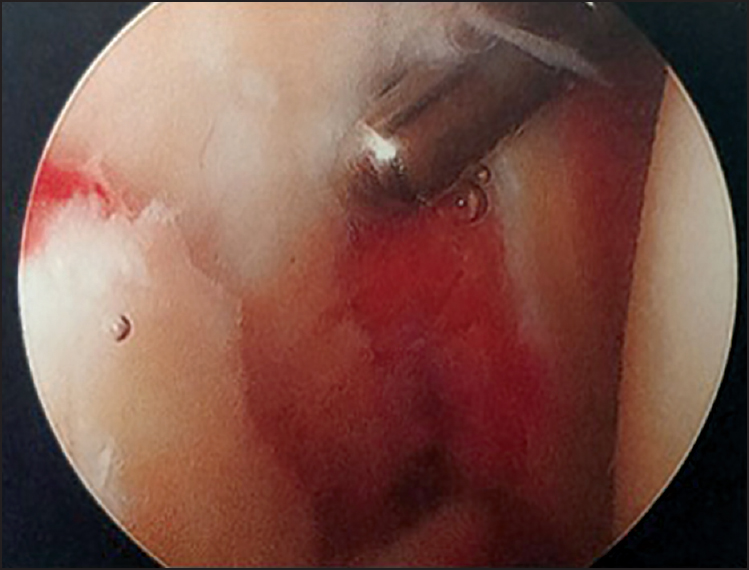 | Figure 3: Intraoperative arthroscopic picture showing the comminuted glenoid fracture with signifi cant articular step. Arthroscopy can allow a much clearer view of the fracture site than is seen in open surgery
Click here to view |
The CT scan had identified the major articular fragment to be continuous with the coracoid. The decision was made to use the coracoid as a joystick to aid indirect reduction. A 3 cm longitudinal skin incision was made directly over the coracoid process. The deltopectoral interval was carefully opened whilst protecting the cephalic vein. The coracoid was then held with a pointed reduction clamp and used as a joystick to manipulate and indirectly reduce the articular surface. Reduction was confirmed with direct visualization of the glenoid via the arthroscope [Figure 4]. A Neviaser's portal was created, and blunt dissection was done down to the glenoid neck. Care was taken not to dissect 1 cm medial to the glenoid neck to avoid suprascapular nerve injury. Two 1.8 mm guide wires were passed through this portal and across the fracture site, under image intensifier guidance. The reduction was monitored using the arthroscope throughout. Intra-articular guide wire penetration was ruled out arthroscopically and radiologically. Care was taken while inserting the guide wires not to progress the wires beyond the inferior cortex of the glenoid neck to avoid injury to the axillary nerve. Two self-drilling and self-tapping BIOMET® UK Ltd (Biomet, Swindon, UK) 4.5 mm cannulated screws were passed over the wires under fluoroscopic guidance, ensuring the screws did not breech the inferior cortex. The screws were tightened sequentially to prevent any rotation of the fragments. A congruent and stable articular reduction was confirmed arthroscopically and radiologically.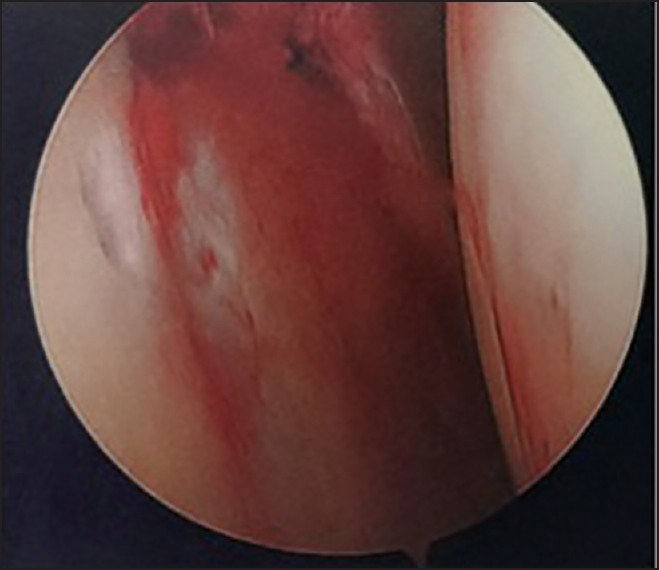 | Figure 4: Arthroscopic image taken after reduction of the glenoid fracture using the coracoid as a reduction tool
Click here to view |
Postoperatively, the shoulder was placed in a sling for 6 weeks with active assisted movements commenced at 3 weeks.
He was seen 2 weeks after surgery in an outpatient clinic, where he was progressing well, with no evidence of suprascapular or axillary nerve deficit. On review, 7 weeks postoperatively, he had returned to all his normal daily activities, including driving. His shoulder movements at 7 weeks were as follows: Forward flexion 170°; abduction 130°; external rotation 30°; internal rotation to L1 level. X-rays revealed fracture union [Figure 5]. | Figure 5: X-rays taken 7 weeks postoperatively show a well-united fracture with adequate articular reduction. Anteroposterior radiograph 7 weeks postoperative
Click here to view |
Due to his remarkable progress, he was discharged from the clinic at this stage, with instructions to return if any problems arise.
| Discussion | | |
Displaced intra-articular glenoid fractures with an articular step over 4 mm or any evidence of glenohumeral instability require anatomical reduction and fixation to avoid early onset glenohumeral arthritis or chronic instability. [1],[6],[7] Traditionally, this has been done via an open approach to allow direct visualization of the articular surface and accurate reduction. The disadvantages of an open technique include: The need for a lot of soft tissue stripping; postoperative weakness; and relatively large incisions. [1],[2],[6],[7] Therefore, recently, there is an increasing trend to fix these fractures via more minimally invasive methods.
In this case, using an arthroscopic assisted technique allowed us to visualize the articular surface while limiting the exposure of the joint to the outside environment. Reduction was achieved using the coracoid process as a joystick to reduce the articular surface under arthroscopic guidance. This proved to be a very convenient and simple reduction tool and to our knowledge, this is the first time this method of reduction has been reported in the literature.
Arthroscopically assisted percutaneous screw fixation has been reported with good results in the literature. [3],[4] Yang et al. reported the results of 18 patients who underwent arthroscopically assisted fixation of Ideberg type III glenoid fractures. They achieved union in all cases with a mean forward flexion, external rotation, and internal rotation of 163°, 67° and level of T8, respectively, at 2 years follow-up. [3] As our patient has already achieved forward flexion, external rotation, and internal rotation of 170°, 30° and level of L1, respectively, just 7 weeks postoperatively, we expect his outcomes will be at least equivalent to Yang's at 2 years. Perhaps more importantly our patient had already returned to all his daily activities at this stage. In Yang's series, only a single cannulated screw was inserted, but considering the comminution of the articular surface in this case, it was felt two screws should be inserted to ensure stable fixation and, therefore, allow early active exercises. [3]
The potential for neurovascular damage during portal, guide wire or screw insertion using this technique has been highlighted in the literature. However, a cadaveric study carried out by Marsland and Ahmed showed that using Neviaser's portal for percutaneous screw insertion is a relatively safe technique, providing the surgeon is aware of the close proximity of the suprascapular nerve and routinely checks this nerve postoperatively. [8] In our case, no neurological deficit was encountered.
| Conclusion | | |
We have described a case of an Ideberg type III glenoid fracture treated successfully using an arthroscopically assisted percutaneous fixation, in which the coracoid was utilized as a novel reduction tool. This technique appears to give a good radiological and functional outcome without the need for extensive soft tissue dissection and is supported by current evidence.
| References | | |
| 1. | Cole PA, Freeman G, Dubin JR. Scapula fractures. Curr Rev Musculoskelet Med 2013;6:79-87.  |
| 2. | Adam FF. Surgical treatment of displaced fractures of the glenoid cavity. Int Orthop 2002;26:150-3. |
| 3. | Yang HB, Wang D, He XJ. Arthroscopic-assisted reduction and percutaneous cannulated screw fixation for Ideberg type III glenoid fractures: A minimum 2-year follow-up of 18 cases. Am J Sports Med 2011;39:1923-8. |
| 4. | Yallapragada R, Patel K, Davuluri P, Sloan A, Marynissen H. Arthroscopy-assisted percutaneous fixation of glenoid fossa fracture. Int J Shoulder Surg 2007;1:96-9.  |
| 5. | Sears BW, Lazarus MD. Arthroscopically assisted percutaneous fixation and bone grafting of a glenoid fossa fracture nonunion. Orthopedics 2012;35:e1279-82. |
| 6. | Anavian J, Gauger EM, Schroder LK, Wijdicks CA, Cole PA. Surgical and functional outcomes after operative management of complex and displaced intra-articular glenoid fractures. J Bone Joint Surg Am 2012;94:645-53. |
| 7. | Schandelmaier P, Blauth M, Schneider C, Krettek C. Fractures of the glenoid treated by operation. A 5- to 23-year follow-up of 22 cases. J Bone Joint Surg Br 2002;84:173-7. |
| 8. | Marsland D, Ahmed HA. Arthroscopically assisted fixation of glenoid fractures: A cadaver study to show potential applications of percutaneous screw insertion and anatomic risks. J Shoulder Elbow Surg 2011;20:481-90. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
|













