| |


 |
| Year : 2015 | Volume
: 9
| Issue : 3 | Page : 90-93 |
|
|
|
|
|
CASE REPORT Sorting swimmers shoulders: An observational study on swimmers that presented to a shoulder surgeon
Daniel Butler1, Len Funk2, Tanya Anne Mackenzie3, Lee C Herrington3
1 The University of Manchester, School of Medicine, Oxford Road, Manchester M13 9PT, United Kingdom
2 Bridgewater Hospital, Manchester Arm Clinic, 120 Princess Road, Manchester, MA15 5AT, United Kingdom
3 University of Salford, College of Health and Social Care, The Crescent, Salford, M5 4WT, United Kingdom
Correspondence Address:
Tanya Anne Mackenzie
University of Salford, The Crescent, Salford, M5 4WT
United Kingdom
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0973-6042.161444
 |
|
|
|
| Date of Web Publication | 24-Jul-2015 |
 Abstract Abstract | | |
Context: It is common for swimmers to suffer shoulder injuries resulting in a wealth of research focusing on the causes and types of injury. However, there is a lack of evidence regarding current management for shoulder injuries in swimmers.
Aims: To investigate the diagnosis, subsequent management, and the return to swimming outcomes for swimmers presenting to an orthopedic practice.
Settings and Design: Retrospective cohort study of competitive swimmers presenting to an orthopedic practice.
Materials and Methods: The diagnosis, subsequent management, and the return to swimming outcomes were analyzed for 14 swimmers whose injuries were managed by a shoulder surgeon.
Statistical Analysis Used: Descriptive analysis.
Results: No significant association was identified between swimming stroke and type of injury. The majority of swimmers had good scapula rhythm, with no visible dyskinesis, including those with impingement. Swimmers with impingement did not require arthroscopy, and with nonoperative management had a mean time to return to swimming of 1.6 months. All labral tears required arthroscopic labral repair, with these swimmers having a mean time of 2.9 months postsurgery to return to swimming.
Conclusion: The study demonstrated that an accurate diagnosis, and appropriate choice of nonoperative and surgical treatments lead to reassuring outcomes for swimmers suffering from shoulder injuries.
Keywords: Impingement, labral, return to swimming, shoulder, swimming
How to cite this article:
Butler D, Funk L, Mackenzie TA, Herrington LC. Sorting swimmers shoulders: An observational study on swimmers that presented to a shoulder surgeon. Int J Shoulder Surg 2015;9:90-3 |
| Introduction | |  |
Swimming is a popular sport across the world, it is reported that 23-38% of competitive swimmers suffer shoulder injuries each year. [1] The upper limbs provide the majority of the propulsion [2] with competitive swimmers achieving over a million repetitive over arm movements annually. [3] Elite swimmers average around 5000 m/training session, training twice a day, 6 to 7 days a week, completing approximately 2500 overhead arm movements a day. [2] Overuse injuries and irritation to the shoulder and surrounding structures can occur as a result. Sein et al., 2010, [4] explain that supraspinatus tendinopathy is a consequence of the vast distances these athletes cover. [4] In the literature, subacromial impingement is the most commonly reported shoulder pathology, and more specifically supraspinatus tendinopathy. [4],[5],[6] Swimmers are also at high risk of developing labral injuries such as superior labral from anterior to posterior (SLAP) tears. [7] Previous literature regarding conservative and surgical treatment of shoulder injuries in swimmers is limited. Current literature describes low return rates to preinjury level for most swimmers. [8],[9] A systematic review by Gaunt and Maffulli, 2012, [6] concluded: There is a "scarcity of recent publications regarding the treatment and rehabilitation of swimming injuries." This study aims to address this "scarcity" in the literature.
| Materials and Methods | | |
A retrospective review was conducted of competitive swimmers presenting to the practice over a 6 years period. Inclusion criteria was a competitive swimmer of club level and above, with a period of failed nonoperative management of more than 6 months prior to referral. Retrospective information was collected on age, gender, level of swimming, preferred stroke, investigations, diagnosis, subsequent management, and time taken to return to swimming. From this data relevant observations and analyses were made regarding the mechanism of injury, diagnoses, management, and return to swimming times.
| Results | | |
Fourteen swimmers met the selection criteria with a mean age of 20 (range: 14-30) years. The group is comprising of nine international athletes, two club level, and three Paralympic swimmers. The predominant stroke of each swimmer was noted with seven swimmers' swimming freestyle, three swimming backstroke, two swimming butterfly, and one swimming breaststroke.
Based on clinical examination including Copeland's, Hawkins Kennedy, Neer's sign, and empty can test, four swimmers were diagnosed with subacromial impingement syndrome and three with internal impingement. The O'Brien's test, Speed's test, Kibler test (or anterior slide), and the crank test (or compression rotation test) were used to diagnose labral injury. Diagnosis of labral injury was confirmed on MR arthrogram imaging and during arthroscopy. Five swimmers had labral tears (two SLAP tears and three Bankart tears). In addition to a SLAP, one swimmer had a HAGL (humeral avulsion of the glenohumeral ligament). One swimmer was diagnosed with multidirectional joint laxity on the drawer tests and sulcus sign.
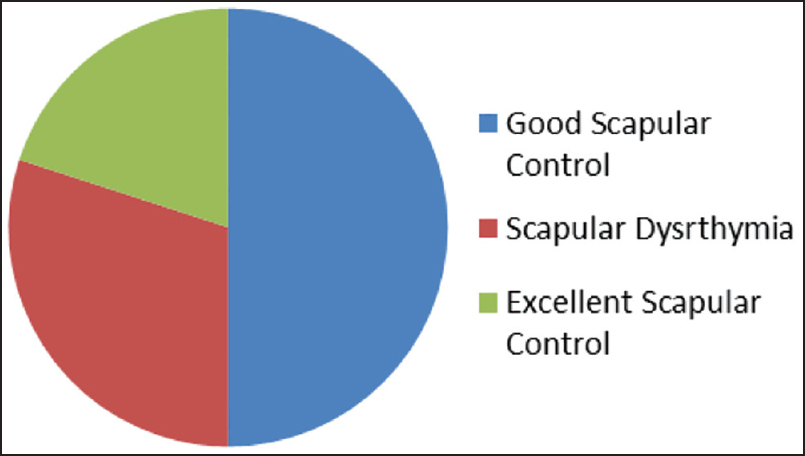
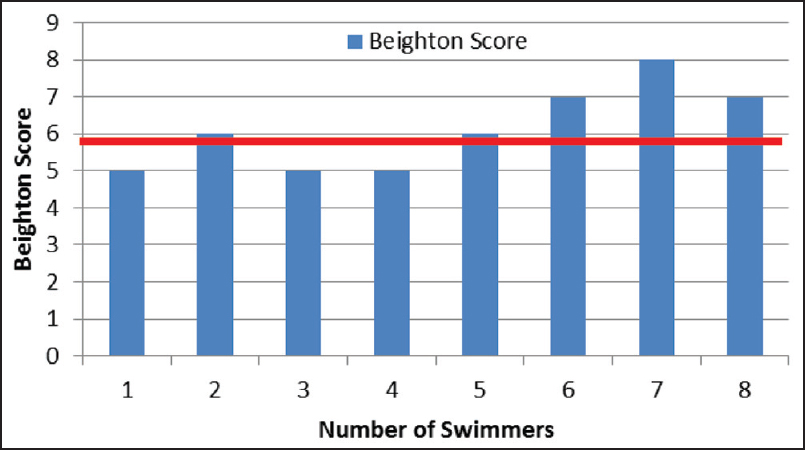
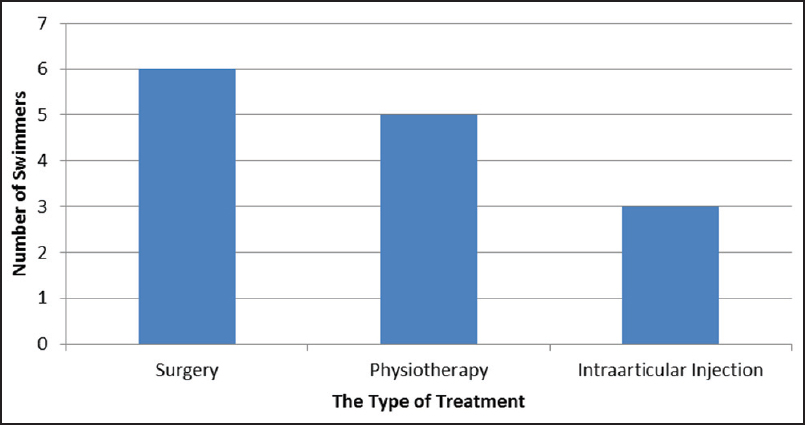
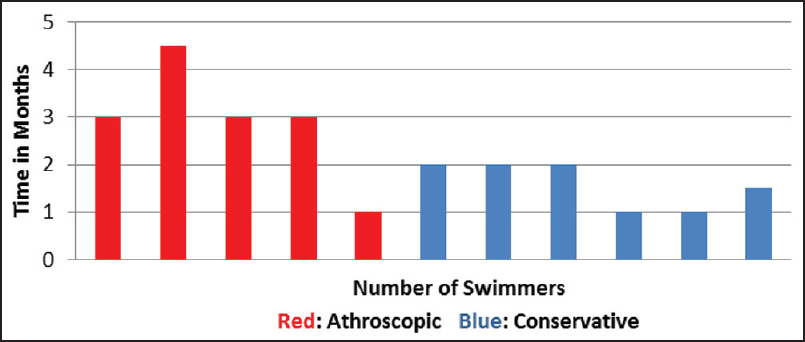
Scapular control was observed in ten swimmers. Five (50%) were recorded as having "good scapular control" (poor resting position of the scapula, but with no scapular dyskinesis on motion), two (20%) had "excellent scapular control" (good scapula resting position with no scapular dyskinesis on motion), and the remaining three swimmers (30%) had "scapular dysrthymia" on examination, as shown in [Figure 1]. Eight of the 14 swimmers had Beighton Scores recorded. Based on the suggested normal threshold of joint laxity in a young athlete of 4-6, [10] three out of eight (37%) athletes tested by the Beighton score had generalized hypermobility. Beighton scores for each swimmer are illustrated in [Figure 2]. All swimmers with impingement signs received conservative treatment, four received physiotherapy alone, and three had intra-articular corticosteroid injections. As illustrated in [Figure 3], six swimmers had surgery. Five with labral pathology underwent arthroscopic labral repair surgery inclusive of: Anterior capsular plication, SLAP repair, capsular shrinkage, Bankart repair, and HAGL repair. The sixth swimmer who underwent surgery had anterior instability and had an arthroscopic anterior capsular shrinkage. There was no outcome data for three swimmers, because one had retired before receiving treatment, another retired as a result of the injury, and one did not attend follow-up appointments. The mean time taken for swimmers who received conservative management inclusive of both physiotherapy and intra-articular injections was 1.6 months compared with 2.9 months in surgical patients [Figure 4].
| Discussion | | |
A study by Wymore et al., 2012, [10] found no correlation between the preferred stroke of the swimmer and development of the shoulder injury. This study supports this finding, with no clear link between swimming stroke and type of injury, although the majority of the swimmers were freestyle swimmers.
Scapular dyskinesias has been associated with an increased likelihood of impingement injuries. [12] Warner et al., 2012, [12] demonstrated scapular dyskinesia in 64% of swimmers with instability and 100% of swimmers with impingement. [12] Madsen et al., 2011, [13] reported 82% of noninjured swimmers had scapular dysrhythmias by the end of a training session, inferring that scapular dysrhythmia may be a normal variant in fatigued swimmers as opposed to a risk factor for shoulder injuries. The majority of swimmers in this study had good scapula rhythm, with no visible dyskinesis, including those in those with chronic impingement. The inconsistency in the literature means future research into the role of scapular control in shoulder injuries in swimmers is required.
The measurement of joint laxity and its usefulness is another area with contrasting discussion. The systematic review by Gaunt and Maffulli, 2012, [6] concluded that joint laxity is a risk factor for injury and warranted further research, and suggested that the Beighton hypermobility grading [6] is appropriate for this. Despite the belief that hyperlaxity is associated with shoulder pathology in the swimming population, only 38% of our swimmers had a score higher than 6 on the Beighton scale. This is similar to the study by Bak 2010, [8] who found a hyperlaxity incidence of 22% in painful swimmers shoulders.
In common with a similar study by Brushøj et al., 2007, [9] labral pathology was a common finding in swimmers shoulders, with impingement signs the second most common finding. Brushøj et al., 2007, [9] reported labral pathology in 69% of cases, in this study 83% of arthroscopic procedures were on labral pathology. In this study, arthroscopic debridement was done and procedures to repair labral pathologies, 50% of which were Bankart tears. This finding differs from the study by Brushøj et al., 2007, [9] who reported to debridement being the most common arthroscopic procedure done on swimmers shoulders, and observed only one Bankart tear in a population of 18 swimmers.
There is little in the literature with regard to HAGAL injuries in swimmers, however the HAGL observed in one swimmer was not attributed to the swimming action, instead the injury occurred when the athlete pushed off the swimming pool wall. This swimmer did not respond to nonoperative therapies and required surgical repair.
The average time is taken to return to swimming training after arthroscopy was 2.9 months, compared with 4 months reported in the study by Brushøj et al., 2007. [9] The return to swimming training and competition data in this study was limited to eleven swimmers. Brushøj et al., 2007, [9] observed that 44% of swimmers who had arthroscopy did not return to swimming. Accurate diagnosis improved selection of swimmers eligible for arthroscopy in this study may have helped improve the success rates.
Improvements in imaging and increasingly specialized physiotherapy mean there are good alternatives to arthroscopy in swimmers with impingement. None of the six swimmers with impingement signs underwent arthroscopy, instead specialist shoulder physiotherapy combined with intraarticular corticosteroid injection, was effective in getting these swimmers back to training. In this study only one athlete, who did not undergo arthroscopy, did not return to swimming because of shoulder pain. A stepwise approach to swimmers presenting with impingement signs should be considered, and nonoperative treatments tried before surgical intervention. Intra-articular injections of steroids can reassure the surgeon to the cause of the swimmer's pain ruling out other possible causes, reducing unnecessary risks of an arthroscopic procedure.
In summary, swimmers with impingement injuries do well with the appropriate nonoperative treatment; however, athletes with labral injuries require surgical intervention.[14]
| References | | |
| 1. | Walker H, Gabbe B, Wajswelner H, Blanch P, Bennell K. Shoulder pain in swimmers: A 12-month prospective cohort study of incidence and risk factors. Phys Ther Sport 2012;13:243-9.  |
| 2. | Pink MM, Tibone JE. The painful shoulder in the swimming athlete. Orthop Clin North Am 2000;31:247-61. |
| 3. | McMaster WC. Shoulder injuries in competitive swimmers. Clin Sports Med 1999;18:349-59, vii. |
| 4. | Sein ML, Walton J, Linklater J, Appleyard R, Kirkbride B, Kuah D, et al. Shoulder pain in elite swimmers: Primarily due to swim-volume-induced supraspinatus tendinopathy. Br J Sports Med 2010;44:105-13. |
| 5. | Tovin BJ. Prevention and treatment of swimmer′s shoulder. N Am J Sports Phys Ther 2006;1:166-75. |
| 6. | Gaunt T, Maffulli N. Soothing suffering swimmers: A systematic review of the epidemiology, diagnosis, treatment and rehabilitation of musculoskeletal injuries in competitive swimmers. Br Med Bull 2012;103:45-88. |
| 7. | Abrams GD, Safran MR. Diagnosis and management of superior labrum anterior posterior lesions in overhead athletes. Br J Sports Med 2010;44:311-8. |
| 8. | Bak K. The practical management of swimmer′s painful shoulder: Etiology, diagnosis, and treatment. Clin J Sport Med 2010;20:386-90. |
| 9. | Brushøj C, Bak K, Johannsen HV, Faunø P. Swimmers′ painful shoulder arthroscopic findings and return rate to sports. Scand J Med Sci Sports 2007;17:373-7. |
| 10. | Wymore L, Reeve RE, Chaput CD. No correlation between stroke specialty and rate of shoulder pain in NCAA men swimmers. Int J Shoulder Surg 2012;6:71-5. [ PUBMED]  |
| 11. | Ellenbecker TS, Cools A. Rehabilitation of shoulder impingement syndrome and rotator cuff injuries: An evidence-based review. Br J Sports Med 2010;44:319-27. |
| 12. | Warner JJ, Micheli LJ, Arslanian LE, Kennedy J, Kennedy R. Scapulothoracic motion in normal shoulders and shoulders with glenohumeral instability and impingement syndrome. A study using Moiré topographic analysis. Clin Orthop Relat Res 1992:191-9. |
| 13. | Madsen PH, Bak K, Jensen S, Welter U. Training induces scapular dyskinesis in pain-free competitive swimmers: A reliability and observational study. Clin J Sport Med 2011;21:109-13. |
| 14. | Beighton P, Solomon L, Soskolne CL. Articular mobility in an African population. Ann Rheum Dis 1973;32:413-8. [ PUBMED] |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|