|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 2
| Issue : 2 | Page : 68-73 |
|
Perception of occlusion and reasons for not seeking orthodontic treatment among Yemeni children
Nabil Muhsen Al-Zubair
Department of Orthodontics, Faculty of Dentistry, Sana'a University, Sana'a, Yemen
| Date of Web Publication | 22-Apr-2014 |
Correspondence Address:
Nabil Muhsen Al-Zubair
Department of Orthodontics, Faculty of Dentistry, Sana'a University, Sana'a
Yemen
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.131116

Aim: The aim of this study was to evaluate perception of the children to their own occlusion and reason for not seeking orthodontic treatment in a sample of 12-year-old Yemeni school children. Materials and Methods: The study sample was comprised of 3003 children, attending schools in six governorates (cities and environs) in Yemen. For each subject, the standard demographic information such as gender and residency was collected, after which a questionnaire was used to determine the perception of occlusion and to assess the history of orthodontic treatment. Results: Of the whole, only 2.2% of the sample had some type of orthodontic treatment or consultation. Nearly 63.4% answered that they have aligned teeth, 29.7% have malaligned teeth, whereas 6.9% of them did not know whether they have aligned or malaligned teeth. Of the children who stated that they have malaligned teeth, 31.6% reported that they had crowded teeth, 15.5% had spaced teeth, 28.5% had protruded teeth and 24.3% had rotated and displaced teeth. Regarding the answers of the effect of malaligned teeth, 60.9% thought that it affects their appearance, 6.5% chewing, and 7.6% speech. The most common reasons for not seeking orthodontic treatment were ignorance about treatment, the thought that treatment is not important or not possible (61.1%) and having fear of pain or tooth extraction (23%). Conclusion: According to the findings of this study, almost 2% of the evaluated Yemeni school children had some type of orthodontic treatment or consultation, suggesting low perception level of the Yemeni children to their own occlusion. Keywords: Occlusion perception, orthodontic treatment, Yemen
How to cite this article:
Al-Zubair NM. Perception of occlusion and reasons for not seeking orthodontic treatment among Yemeni children. J Orthod Res 2014;2:68-73 |
How to cite this URL:
Al-Zubair NM. Perception of occlusion and reasons for not seeking orthodontic treatment among Yemeni children. J Orthod Res [serial online] 2014 [cited 2018 Mar 1];2:68-73. Available from: http://www.jorthodr.org/text.asp?2014/2/2/68/131116 |
| Introduction | |  |
Studying the prevalence of malocclusion and assessment of treatment needs in a community are important steps in planning orthodontic services. It is also equally important to study the demand for this service. Demand for treatment generally depends on the awareness and perception of the problem of malocclusion, because not all patients with malocclusion seek orthodontic treatment. [1]
Many studies in this field concluded that the desire to improve appearance is the most important motive for seeking treatment, while other studies concentrated on the effect of malocclusion on functions like speech and mastication. [2],[3],[4],[5],[6]
Consumers perceived needs (wants) are based on their awareness of potential disease and on personal experience and depend on culture, religious, educational and social status. As such, they are an important determinant of consumer behavior, i.e., a determinant of what economists call demand. [7]
Studies on perception of malocclusion discussed the effects of various factors on the awareness of occlusal anomalies and the demand for treatment; among these factors are:
- Types of occlusal anomalies that lead to awareness and demand for treatment: Various studies have been conducted to assess which types of occlusal anomalies cause more concern to the patient. [5],[8],[9],[10],[11],[12],[13],[14]
- Gender: Some studies concluded that the awareness of malocclusion and demand for treatment is more in females than males. [3],[9],[15] Furthermore, women were found to be more dissatisfied with their dental appearance. [16],[17] Other studies did not show significant differences between males and females in esthetic preference and concern over appearance. [5],[18]
- Age: In some studies, the effect of age as a factor on judgment of facial attractiveness was found to be insignificant. [15] It was also not significant in the reliability and accuracy of identification of malocclusion, [5] while other studies showed that dissatisfaction with dental appearance increases with age. [10],[16]
- Socio-cultural factors: Studies have shown that people generally under estimate their malocclusion, creating a gap between need and demand. However, most of these studies stress on the effect of social factors on treatment demand. [6],[10],[12],[19] High social classes place greater value on facial appearance and this increases their demand for treatment; [1],[15] while in a study by Shaw [16] it was stated that dissatisfaction with dental appearance was not associated with social class.
Methods of studying perception of occlusion can be divided into two main types: (1) Questionnaires: This method is used to assess the individual's perception of his or her occlusion by comparing the answers with an objective assessment of the individual's occlusal status. [5],[8],[11],[17],[20] In some studies on children's perception of occlusion, the questionnaires were answered by the child and her or his parents. [6],[12] (2) Photographs: In studies employing this method the participants were either asked to identify their photograph from a series of photographs of teeth, or in some studies the participants were asked to rate a series of photographs of teeth according to their attractiveness. [16],[19],[21] In some studies this method was modified by using slides instead of photographs. [22]
Studying perception of occlusion and awareness of malocclusion is important in planning health services on a community as well as on individual's level, because the patient's own image is part of the behavioral history and affects the patient's cooperation. [23]
| Materials and Methods | | |
The sample was comprised of 3071, 12-year-old children attending schools in six governorates (cities and environs) in Yemen.
In each governorate, the same multi-stage stratified sampling technique was implemented. From each sector, 500 children were included in the survey, half of whom were urban and the other half were rural.
Urban children were considered as those living in the center of each governorate taken as clusters of 25 students from 10 randomly selected schools. Rural children were selected from five small villages from each sector, two clusters of 25 students from each village.
This gives a total of 3003 children taken from 120 schools; 1501 of whom were females. The number of children examined was increased more than planned to adjust for those who were excluded due to history or those who were currently undergoing orthodontic treatment or undergone extraction of permanent teeth to improve the appearance.
From each school, the first accessible 25 children were examined. A total of 13 schools did not have 25 children of 12-years of age so neighboring schools were visited to complete the required number making the total number of 133 schools visited.
Permission was obtained from the general directorate of education in Yemen and the regional directorate of education in the governorates. All school authorities were contacted and the aim of the present study was explained to them to ensure full cooperation.
Questionnaire
Before performing the questionnaire, the date of examination, the name of governorate, residency, school, school class and gender of the children was registered, after which a questionnaire was used to determine the perception of occlusion. This questionnaire was modified from the questionnaire of Ingervall et al. and Ng'ang'a et al. [10],[24] and translated to the Arabic language. The questions were as follows:
1. Do you find that your teeth are irregular (not straight) or come together in a wrong way?
(a) Yes, (b) No, (c) Do not know
2. If yes, do you think that your teeth are:
(a) Crowded, (b) spaced, (c) protruded, (d) rotated or displaced.
3. If your teeth are irregular, does this affects your:
(a) Appearance, (b) chewing or mastication, or (c) speech and pronunciation.
4. If you think you need orthodontic treatment, why have you not done so yet, is it because you think that the treatment is:
(a) Not possible, (b) expensive, (c) painful, (d) not important, or (e) another reason (mention it).
The children with signs of orthodontic treatment were also asked about any previous history of orthodontic treatment:
- Have you ever had orthodontic treatment in the past (describe the type of treatment)?
- Are you currently under orthodontic treatment (describe type of treatment and appliance)?
- Has any of your teeth been extracted to improve appearance (which one(s))?
Statistical Analysis
All statistical analyses were performed using SPSS 13.0. Pearson's Chi-square test was used to test the differences between the sexes and the degree of urbanization. Statistical significance was predetermined at the 95% level (P < 0.05).
| Results | | |
[Table 1] depicts a history of orthodontic treatment. Only 2.2% of the sample either undergone or undergoing orthodontic treatment (0.9%) or extracted teeth to improve appearance (1.3%), while the majority of the sample (97.8%) did not undergoing orthodontic treatment.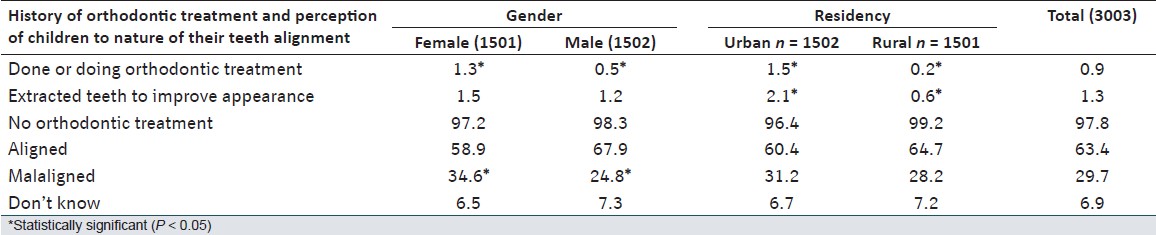 | Table 1: Distribution of the history of orthodontic treatment and perception of children to nature of their teeth alignment according to gender and residency
Click here to view |
Considering gender differences, statistically significant difference was reported between female and male; which the rate of undergone or undergoing orthodontic treatment in female was more than male (χ2 = 12.278, df = 1, P < 0.05).
Orthodontic extractions were found to be more in urban (2.1%) compared with rural children (0.6%). This difference was statistically significant (χ2 = 63.472, df = 1, P < 0.05).
The perception of children to nature of their teeth alignment is shown also in [Table 1]. Of whom, 63.4% answered that they have aligned teeth, 29.7% answered that they have malaligned teeth, while 6.9% of them did not know whether they have aligned or malaligned teeth. The number of the females answered that they have malaligned teeth (34.6%) was more than that in the males (24.8%), this results was statistically significant (χ2 = 50.802, df = 1, P < 0.05).
[Table 2] depicts the perception of children who answered that they have malaligned teeth toward the type of malalignment. 282 children (31.6%) had crowded teeth, 140 students (15.5%) had spaced teeth, 255 children (28.5%) had protruded teeth and 215 children (24.3%) had rotated and displaced teeth.
The answers of children to effect of malalignment are also demonstrated in [Table 2]. Of the 892 children who stated that they have malaligned teeth, 543 children (60.9%) thought that it affects their appearance, 58 children (6.5%) chewing and 68 children (7.6%) speech, while 223 children (25%) answered that malaligned teeth did not affect their appearance, chewing or speech.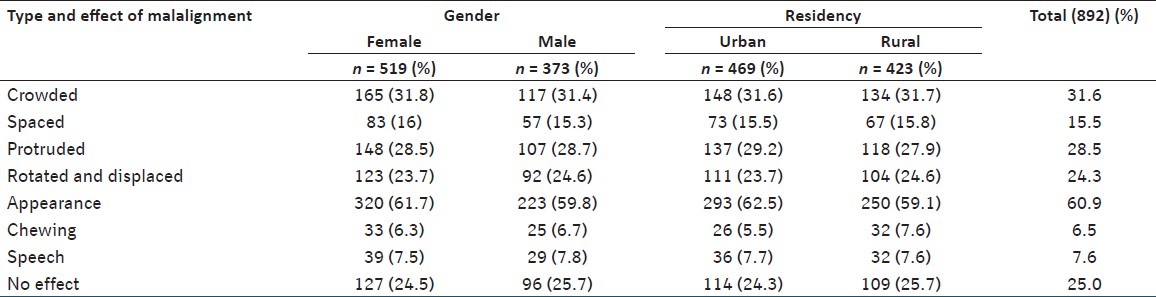 | Table 2: Distribution of the perception of children toward type and effect of malalignment
Click here to view |
The reasons for not seeking orthodontic treatment in spite of their belief that they had malaligned teeth are shown in [Table 3]. Of whom, 27.1% did not know about orthodontic treatment, 17.5% said that treatment is not important, 16.5% thought that treatment is not possible, 14.1% feared for pain, and 8.9% feared for extraction of teeth. Other less popular reasons included: Hope for spontaneous improvement (6.6%), treatment is expensive (4.5%), no time for treatment (2.4%), poor esthetics of appliances (1.1%), postponed by the dentist (0.6%), difficult to get used to orthodontic appliances (0.5%), and fear of cross contamination (0.2%).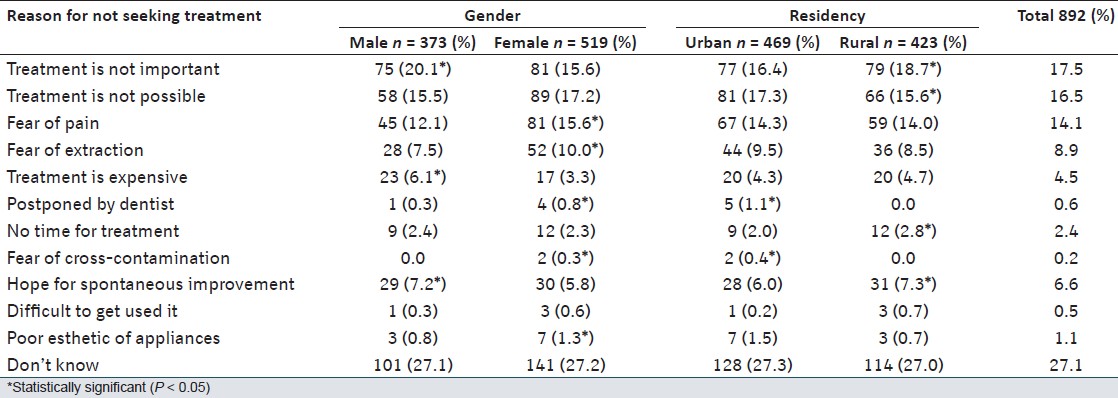 | Table 3: Distribution of the answers regarding reasons for not seeking treatment
Click here to view |
The number of the females answered that they had a fear of pain, fear of extraction, postponed by the dentist, fear of cross-contamination, difficulties to get used to it and concern about poor esthetics of appliances was more than that in the males, while the number of the males answered that treatment is not important or expensive, they had a hope for spontaneous improvement was more than the female. This result was statistically significant (χ2 = 22.577, df = 9, P < 0.05).
The number of the urban children answered that they had postponed by the dentist and fear of cross-contamination was more than the number of the rural students, while the number of the rural children answered that treatment is not important or not possible, no time for treatment, they had a hope for spontaneous improvement, and difficulties to get used to it was more than the number of the urban children. This result was statistically significant for the male sample (χ2 = 43.482, df = 9, P < 0.05).
| Discussion | | |
Before discussing the four questions regarding the awareness of malocclusion it may be better to discuss the three questions regarding the past and present orthodontic treatment of the children.
Of the total sample, 0.9% undergone or undergoing orthodontic treatment, 1.3% had undergone extractions to improve the appearance and 0.5% reported that their treatment was postponed by a dentist for a later time; giving a total of 2.7% of the sample who have had some type of orthodontic treatment or consultation. The percentage was very small when compared to studies carried out in European countries as Sweden, Denmark and Finland which show that about 27-45% of their samples have received some sort of orthodontic treatment. [25],[26],[27],[28],[29]
On the other hand, Al-Huwaizi [14] found that 3.2% of his sample had some type of orthodontic treatment or consultation and this figure was close to ours. The scarcity of orthodontic treatment may be explained by the small number of dentist in general and orthodontic specialists in specific in Yemen and the lack of a health insurance system concerned with orthodontic treatment in Yemen.
Females showed higher rate of orthodontic treatment (appliances or extraction) than males in accordance with Al-Huwaizi, [14] which may be resulted from the fact that females are more concerned with their appearance than males.
Orthodontic treatment rate (appliances or extraction) was found to be higher in the urban sample than that in the rural sample. This may be explained by the fact that all orthodontic specialists in Yemen reside and practice in the large cities making it more difficult for rural children to obtain treatment.
Regarding the self-evaluation of the children to the alignment of their teeth, 29.7% of them answered that they have malaligned teeth. This rate was similar to that found by Salonen et al. in Sweden [30] but less than that of Ingervall et al. in Sweden [10] and Ng'ang'a et al. in Kenya. [24]
The awareness of malocclusion was significantly high in females than males, which is similar to the findings of Salonen et al. [30] This again may be resulted from the fact that females are more concerned with their appearance than males. However, Ng'ang'a et al. [24] found no significant difference between sexes about this result which may be attributed to cultural and/or social differences.
Concerning the type of malaligned teeth, the children reported their malocclusion type as follows with descending sequence of prevalence crowded, protruded, rotated and displaced teeth and spaced teeth. This sequence is different from that of Abdulla [11] and others, but identical to the findings of Graber and Lucker [13] and Al-Huwaizi. [14]
Of the 892 children who stated that they have malaligned teeth, 61.3% thought that it affected their appearance, 6.8% chewing and 7.7% speech, while 24.9% answered that malaligned teeth did not affect appearance, chewing or speech. This result is comparable to that found by Batayine [8] in Jordan and Al-Huwaizi [14] in Iraq.
The most common reason for not seeking orthodontic treatment was that the children didn't know about orthodontic treatment, treatment is not important, treatment is not possible, had a fear of pain and fear of tooth extraction. The predominance of fear of pain is similar to that of Batayine, [8] Al-Huwaizi [14] and Gatchel. [31]
About two-thirds of the sample didn't know presence of orthodontic treatment or believed that treatment is not possible or not important. This is a communal problem and could be solved by education of the community through the media or public dental health education programs.
| Conclusions | | |
- The presence of malaligned teeth was reported by 29.7% of the sample, being more in female and more in Sana'a and Aden. The most prevalent reported types of malaligned teeth were crowded and protruded teeth.
- Of the children who stated that they have malaligned teeth, 60.9% thought that it affects their appearance 6.5% chewing, and 7.6% speech.
- The most common reasons for not seeking orthodontic treatment were ignorance about treatment, the thought that treatment is not possible or not important (61.1%) and having fear of pain or tooth extraction (23%).
| References | | |
| 1. | Graber TM, Swain BF. Orthodontics-Current Principles and Techniques. St. Louis: C.V. Mosby Co.; 1985. 
|
| 2. | Salzmann JA. Malocclusion severity assessment. Am J Orthod 1967;53:109-19.
[PUBMED] |
| 3. | Mohlin B. Need and demand for orthodontic treatment in a group of women in Sweden. Eur J Orthod 1982;4:231-42.
[PUBMED] |
| 4. | Jacobson A. Psychological aspects of dentofacial esthetics and orthognathic surgery. Angle Orthod 1984;54:18-35.
[PUBMED] |
| 5. | Helm S, Kreiborg S, Solow B. Psychosocial implications of malocclusion: A 15-year follow-up study in 30-year-old Danes. Am J Orthod 1985;87:110-8.
[PUBMED] |
| 6. | Gosney MB. An investigation into some of the factors influencing the desire for orthodontic treatment. Br J Orthod 1986;13:87-94.
[PUBMED] |
| 7. | Van Wyk PJ, van Rooy HK, Rudolph MJ, van der Merwe CA. Unmet and Illmet Demand for Oral Health Services in the RSA. In: Van Wyk PJ, editor. Results of the National Oral Health Survey: South Africa 1988/89;1994. p.147-52.
|
| 8. | Batayine FA. Occlusal features and perception of occlusion of Jordanian adolescents: A comparative study with an Iraqi sample. Master Thesis. Iraq: College of Dentistry, University of Baghdad; 1997.
|
| 9. | Foster TD, Day AJ. A survey of malocclusion and the need for orthodontic treatment in a Shropshire school population. Br J Orthod 1974;1:73-8.
[PUBMED] |
| 10. | Ingervall B, Mohlin B, Thilander B. Prevalence and awareness of malocclusion in Swedish men. Community Dent Oral Epidemiol 1978;6:308-14.
[PUBMED] |
| 11. | Abdulla NM. Occlusal features and perception: A sample of 13-17 years old adolescents. Master Thesis. Iraq: College of Dentistry, University of Baghdad; 1996.
|
| 12. | Lindsay SJ, Hodgkins JF. Children′s perceptions of their own malocclusions. Br J Orthod 1983;10:13-20.
[PUBMED] |
| 13. | Graber LW, Lucker GW. Dental esthetic self-evaluation and satisfaction. Am J Orthod 1980;77:163-73.
[PUBMED] |
| 14. | Al-Huwaizi AF. Occlusal features, perception of occlusion, orthodontic treatment need and demand among 13-year-old Iraqi school children. Doctorate Thesis. Iraq: College of Dentistry, University of Baghdad; 2002.
|
| 15. | Baldwin DC. Appearance and aesthetics in oral health. Community Dent Oral Epidemiol 1980;8:244-56.
[PUBMED] |
| 16. | Shaw WC. Factors influencing the desire for orthodontic treatment. Eur J Orthod 1981;3:151-62.
[PUBMED] |
| 17. | Neumann LM, Christensen C, Cavanaugh C. Dental esthetic satisfaction in adults. J Am Dent Assoc 1989;118:565-70.
|
| 18. | De Smit A, Dermaut L. Soft-tissue profile preference. Am J Orthod 1984;86:67-73.
[PUBMED] |
| 19. | Tulloch JF, Shaw WC, Underhill C, Smith A, Jones G, Jones M. A comparison of attitudes toward orthodontic treatment in British and American communities. Am J Orthod 1984;85:253-9.
[PUBMED] |
| 20. | Katz RV. Relationships between eight orthodontic indices and an oral self-image satisfaction scale. Am J Orthod 1978;73:328-34.
[PUBMED] |
| 21. | Jenny J, Cons NC, Kohout FJ, Frazier PJ. Test of a method to determine socially acceptable occlusal conditions. Community Dent Oral Epidemiol 1980;8:424-33.
[PUBMED] |
| 22. | Cons NC, Jenny J, Kohout FJ, Freer TJ, Eismann D. Perceptions of occlusal conditions in Australia, the German Democratic Republic and the United States of America. Int Dent J 1983;33:200-6.
[PUBMED] |
| 23. | Proffit WR, Ackerman JL. Rating the characteristics of malocclusion: A systematic approach for planning treatment. Am J Orthod 1973;64:258-69.
[PUBMED] |
| 24. | Ng′ang′a PM, Stenvik A, Ohito F, Ogaard B. The need and demand for orthodontic treatment in 13- to 15-year-olds in Nairobi, Kenya. Acta Odontol Scand 1997;55:325-8.
|
| 25. | Helm S. Malocclusion in Danish children with adolescent dentition: An epidemiologic study. Am J Orthod 1968;54:352-66.
[PUBMED] |
| 26. | Helm S, Kreiborg S, Barlebo J, Caspersen I, Eriksen JH, Hansen W, et al. Estimates of orthodontic treatment need in Danish schoolchildren. Community Dent Oral Epidemiol 1975;3:136-42.
[PUBMED] |
| 27. | Bernhold M, Lindqvist B. Orthodontic care in the Swedish Public Dental Service, county of Västerbotten. Swed Dent J 1981;5:105-13.
[PUBMED] |
| 28. | Rölling S. Orthodontic treatment and socioeconomic status in Danish children aged 11-15 years. Community Dent Oral Epidemiol 1982;10:130-2.
|
| 29. | Pietilä T, Pietilä I. Adolescents′ concern for dental appearance in a medium sized Finnish community. Eur J Orthod 1993;15:342.
|
| 30. | Salonen L, Mohlin B, Götzlinger B, Helldén L. Need and demand for orthodontic treatment in an adult Swedish population. Eur J Orthod 1992;14:359-68.
|
| 31. | Gatchel RJ. The prevalence of dental fear and avoidance: Expanded adult and recent adolescent surveys. J Am Dent Assoc 1989;118:591-3.
[PUBMED] |
[Table 1], [Table 2], [Table 3]
|










 Search Pubmed for
Search Pubmed for