|
 
 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 3
| Issue : 1 | Page : 57-60 |
|
Orthodontic camouflage treatment in skeletal Class II patient
MB Raghuraj1, Rajat Scindhia1, Vivek Amin2, Sandeep Shetty2, Rohan Mascarenhas2, Nandish Shetty2
1 Departments of Orthodontics and Dentofacial Orthopaedics, Dr. Syamala Reddy Dental College Hospital and Research Centre, Munnekolala, Marathahalli, Bengaluru, India
2 Yenepoya Dental College, Mangalore, Karnataka, India
| Date of Web Publication | 29-Dec-2014 |
Correspondence Address:
M B Raghuraj
Department of Orthodontics and Dentofacial Orthopaedics, Dr. Syamala Reddy Dental College Hospital and Research Centre, #111/1, SGR College Main Road, Munnekolala, Marathahalli (post), Bengaluru - 560 037, Karnataka
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.146354

Orthodontic camouflage is a method of correcting malocclusion without involving the correction of skeletal problem. Planned extraction of some teeth will help us achieve favorable dental occlusion. The challenge lies in proper diagnosis and case selection so as to decide on dental camouflage as a treatment option in skeletal discrepancy cases. Case of Class II malocclusion with severe crowding, vertical growth pattern and Class II skeletal base with ANB 6° has been discussed. Treated with four premolar extractions and finished the case with Class I canine and molar relationship. Planned extraction of indicated teeth to bring about dental compensation and camouflage the underlying skeletal discrepancy gives an overall improvement in facial esthetics, occlusion and also satisfaction to the patient. Keywords: Malocclusion, crowding and orthodontics
How to cite this article:
Raghuraj M B, Scindhia R, Amin V, Shetty S, Mascarenhas R, Shetty N. Orthodontic camouflage treatment in skeletal Class II patient. J Orthod Res 2015;3:57-60 |
How to cite this URL:
Raghuraj M B, Scindhia R, Amin V, Shetty S, Mascarenhas R, Shetty N. Orthodontic camouflage treatment in skeletal Class II patient. J Orthod Res [serial online] 2015 [cited 2018 Sep 6];3:57-60. Available from: http://www.jorthodr.org/text.asp?2015/3/1/57/146354 |
| Introduction | |  |
Orthodontic camouflage is a method of correcting malocclusion by making the skeletal problem less apparent. Planned extraction of some teeth will help us achieve favorable dental occlusion. The challenge lies in proper diagnosis and case selection so as to decide on dental camouflage as a treatment option in skeletal discrepancy cases. Class II malocclusions can be treated by several means, according to the characteristics associated with the problem, such as anteroposterior discrepancy, age, and patient compliance. [1] Methods include extraoral appliances, functional appliances and fixed appliances associated with Class II intermaxillary elastics. [2]
The purpose of this report is to describe case selection and diagnosis of a Class II malocclusion with Class II skeletal base, which has been treated by way of orthodontic camouflage.
| Case Report | | |
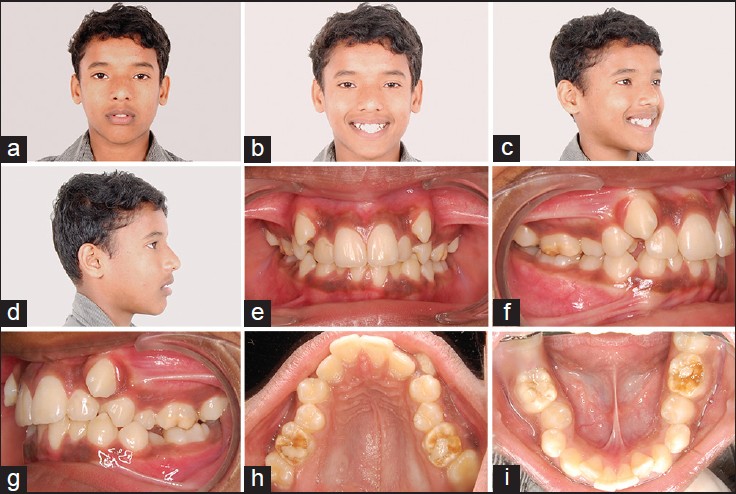
A 13-year-old male patient presented with a chief complaint of irregularly placed upper and lower front teeth. Clinical examination revealed severe crowding in the maxillary arch of 16 mm and crowding in the mandibular arch of 8 mm [Figure 1]a-i, pretreatment photographs]. The molar relation was full cusp Class II on both side, highly placed maxillary canine on both side and lingually erupting mandibular second premolars.
The maxillary incisors showed 5 mm exposure at rest, and lower incisors were upright. An overbite of approximately 4 mm and overjet of 3 mm was noted. The midlines are coinciding with each other and also with skeletal midline. Labial gingival recession was noted in relation to 31, localized pitting type of fluorosis was noted in relation to all the first molars, which have been restored temporarily.
The extra oral photographs show convex profile with retrognathic mandible and mild incompetency with lips. Lower anterior facial height (LAFH) was excessive and upper lip length was considered normal. Skeletal analysis as obtained by cephalometric assessment of patient's lateral head film showed a Class II skeletal pattern and vertical growth pattern with ANB of 6° [Figure 2]a and b, pretreatment radiographs]. | Figure 2: (a and b) Pretreatment lateral cephalogram and orthopantomogram
Click here to view |
Treatment Objectives
- Correction of crowding in both the arches.
- Correction of overjet and overbite.
- Achieve a Class I molar and canine relationship on both side.
- Crown placement on all first molars after completion of orthodontic treatment.
Correction of skeletal Class II relation was not considered in this case, as reasons being; excessive vertical growth pattern, which would increase if mandibular advancement or distalization in the maxillary arch is planned. LAFH would also increase and hamper the overall esthetics of the patient.
Treatment Plan
Based on the tooth size and arch length discrepancy, it was decided to go with extraction of both maxillary first premolars and both mandibular second premolars. Space requirement in the maxillary arch was in anterior segment hence extraction space was utilized to relieve crowding. Space requirement in the lower arch was in the posterior segment hence extraction space was utilized for mesial movement of the molars.
Course of Treatment
The treatment was progressed with extraction of indicated teeth and MBT appliance prescription with 0.022 inch slot was bonded and bands were cemented on molars. Bracket placement was performed using modified bracket positioning holder. [3] Active lacebacks were given on all four quadrants; initial archwire used was 0.14 nickel titanium on both the arch.
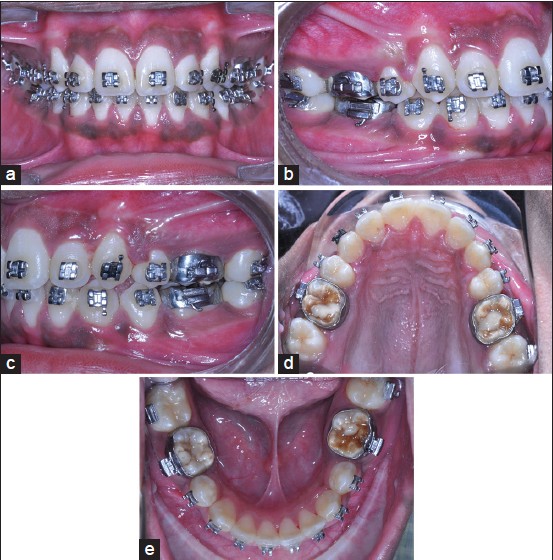
Archwire sequencing was followed by 0.016, 0.018, 0.017 × 0.025 and 0.019 × 0.025inch nickel titanium and working wire of 0.019 × 0.025inch stainless steel. Alignment was completed in 12 months in the maxillary arch and 8 months in the mandibular arch. Mesial movement of mandibular molars was carried out with active tie backs and Class II elastics. Class II elastics were used judiciously to aid in protraction of mandibular molars. Space closure in the mandibular arch was completed in 7 months [Figure 3]a-e, mid treatment photographs].
As extraction pattern was maxillary first premolar and mandibular second premolars, there was a difference of the amount of tooth material in both the arch. The mandibular second premolars were meisodistally larger than maxillary first premolar, hence inter proximal reduction was carried out to correct the tooth ratio in the maxillary posterior region. Finishing and detailing was carried out for 2 months, and the case was finished with Class I canine and molar relationship with optimum overjet and overbite [Figure 4]a-i, posttreatment photographs].
| Discussion | | |
Treatment of any Class II patient requires careful diagnosis and a treatment plan involving esthetic, occlusal and functional considerations. [4] When planning treatment in such cases, the orthodontist often faces the dilemma whether to go with extraction plan [5] or mandibular advancement plan or distalization of maxillary arch in growing patients or surgical correction in case of adult patients. The indications for extractions in orthodontic practice have historically been controversial. [6],[7],[8] For correction of Class II malocclusions extractions can involve two maxillary premolars [9] or two maxillary and two mandibular premolars. [10] In the present case, it was very critical to decide about the extraction pattern and treatment plan as the patient was in a growing age group. Cephalometric analysis confirmed the diagnosis of skeletal Class II relation with ANB of 6°. Surgical correction of the mandible was also ruled out based on the age group.
With an ANB of 6° and growing age group, it is ideal to take advantage of the residual growth and correct the jaw discrepancy by considering functional jaw orthopedics. However in this case, none of these options were suitable and hence extractions were planned, and dental camouflage was decided based on the reasons been explained earlier.
During the treatment, progression anchorage was one more integral part of the treatment which had to be planned. In this case, only light continuous force was used so as to close the extraction space. This helped in reducing the load over the anchor segment (posterior segment in the maxillary arch and first premolar to first premolar in the mandibular arch) and thereby reducing anchorage requirement. The anchorage was reinforced by including second permanent molar in the maxillary arch and all the anchor segments were consolidated together by figure eight ligation.
There is a tendency for the mandible to be displaced mesially during treatment in extraction case more so than nonextraction case. [11] Based on the mandibular second premolar extraction in this case, we expected changes in the molar relationship by mesialization of molars which also helped in reducing the LAFH and as well as reduce ANB value from 6° to 4°. Mesialization of lower molars in this case also helped to create space for the erupting third molars and avoid impaction of mandibular third molars.
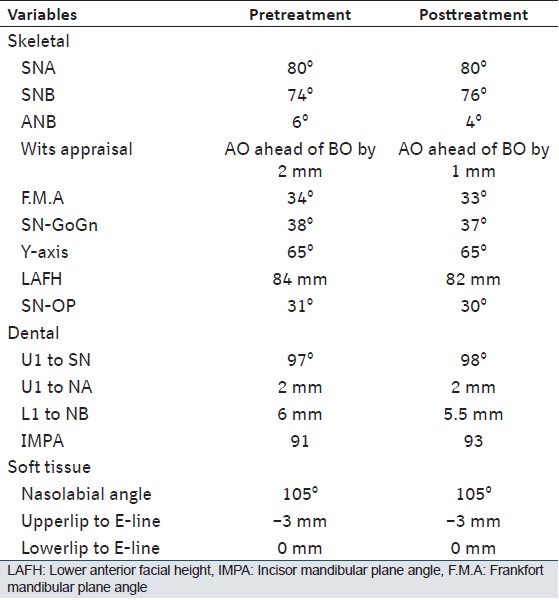
According to Steiner's analysis upper and lower incisor relationship is expected to be at a particular position when the ANB is of 4° as represented graphically in "Steiner Sticks" or "Chevron's" to achieve normal occlusion. [12] The posttreatment values of the present case showed similar compromised values of upper and lower incisor with an ANB of 4° [Table 1].
Finishing and detailing was carried out in 0.014 inch nickel titanium archwire. [13] Occlusal settling was completed by using settling elastics. Posttreatment radiographs were taken immediately prior to debonding, to assess the root positioning [Figure 5]a and b, posttreatment radiographs]. The case was debonded and maxillary removable wrap around retainer was placed to aid in further settling, and lingual 3-3 fixed retainer in the mandibular arch was bonded.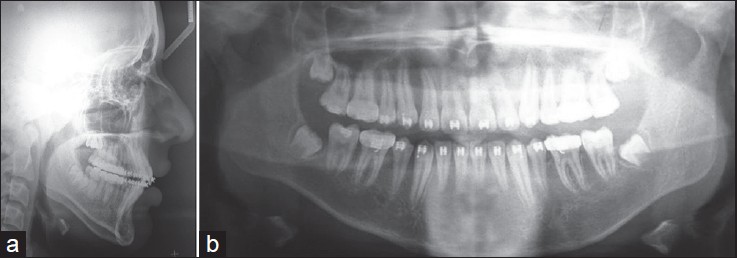 | Figure 5: (a and b) Posttreatment lateral cephalogram and orthopantomogram
Click here to view |
| Conclusion | | |
Orthodontic camouflage treatment in Class II patient is challenging, unless proper diagnosis and treatment plan is laid down. Planned extraction of indicated teeth to bring about dental compensation and camouflage the skeletal discrepancy gives an overall improvement in facial esthetics, occlusion and also satisfaction to the patient.
| Acknowledgment | | |
The first author would like to thank Dr. Akhter Husain, Professor and Head Department of Orthodontics and other teaching and nonteaching Faculty of Orthodontics Department, Yenepoya Dental College at the Yenepoya University of Mangalore for all the support with the case study.
| References | | |
| 1. | Salzmann JA. Practice of Orthodontics. Philadelphia: J. B. Lippincott Company; 1966. p. 701-24.  |
| 2. | McNamara JA Jr. Components of class II malocclusion in children 8-10 years of age. Angle Orthod 1981;51:177-202. [ PUBMED] |
| 3. | Raghuraj MB, Shetty N, Sharan. Modified bracket positioning holder. Contemp Clin Dent 2011;2:142. [ PUBMED]  |
| 4. | Kuhlberg AJ, Glynn E. Treatment planning considerations for adult patients. Dent Clin North Am 1997;41:17-27. |
| 5. | Sood S. Treatment of Class II division 1 malocclusion in a non growing patient virtual. J Orthod 2010;8:3. |
| 6. | Case CS. The question of extraction in orthodontia. Am J Orthod 1964;50:660-91. |
| 7. | Case CS. The extraction debate of 1911 by Case, Dewey, and Cryer. Discussion of case: The question of extraction in orthodontia. Am J Orthod 1964;50:900-12. |
| 8. | Tweed CH. Indications for the extraction of teeth in orthodontic procedure. Am J Orthod Oral Surg 1944;42:22-45. [ PUBMED] |
| 9. | Cleall JF, BeGole EA. Diagnosis and treatment of class II division 2 malocclusion. Angle Orthod 1982;52:38-60. [ PUBMED] |
| 10. | Strang RHW. Treaty of orthodontics. Buenos Aires: Editorial Bibliogra'fica. Argentina. 1957; 560-70:657-71. |
| 11. | Luppanapornlarp S, Johnston LE Jr. The effects of premolar-extraction: A long-term comparison of outcomes in "clear-cut" extraction and nonextraction Class II patients. Angle Orthod 1993;63:257-72. |
| 12. | Steiner CC. The use of cephalometrics as an aid to planning and assessing orthodontic treatment. Am J Orthod 1960;46:721-35. |
| 13. | McLaughlin RP, Bennet JC, Trevisi HJ. Systemized Orthodontic Treatment Mechanics. Edinburgh: Mosby; 2001. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
[Table 1]
|











 Search Pubmed for
Search Pubmed for