|
 
 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 3
| Issue : 1 | Page : 61-64 |
|
Management of maxillary lateral incisor: Canine transposition along with maxillary canine impaction on the contralateral side
Veerendra Prasad1, Pradeep Tandon2, Gyan Prakash Singh2, Rana Pratap Maurya3
1 Department of Plastic Surgery, King George's Medical University (Erstwhile K.G.M.C.), Lucknow, Uttar Pradesh, India
2 Department of Orthodontics and Dentofacial Orthopaedics, King George's Medical University (Erstwhile K.G.M.C.), Lucknow, Uttar Pradesh, India
3 Department of Orthodontics and Dentofacial Orthopedics, Babu Banarasi Das College of Dental Sciences, Lucknow, Uttar Pradesh, India
| Date of Web Publication | 29-Dec-2014 |
Correspondence Address:
Veerendra Prasad
Department of Plastic Surgery, King George's Medical University, Lucknow - 226 003, Uttar Pradesh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.146357

This is a case of 24 years 5-month-old female whose chief complaint was irregularly arranged front teeth. The clinical and radiographical examination revealed pleasing profile, Angle's Class I molar relationship, complete transposition of maxillary right lateral incisor and canine along with impacted left maxillary canine and retained deciduous canine. Maximal band tension 0.022″ × 0.028″ appliance was placed. Transposed right maxillary canine and lateral incisor as well as impacted left maxillary canine was aligned in the dental arch. The total treatment time taken was 24 months, which was followed by a lingual-bonded canine-to-canine retainer. Keywords: Maxillary canine impaction, transposition of maxillary canine-lateral incisor, power arm
How to cite this article:
Prasad V, Tandon P, Singh GP, Maurya RP. Management of maxillary lateral incisor: Canine transposition along with maxillary canine impaction on the contralateral side. J Orthod Res 2015;3:61-4 |
How to cite this URL:
Prasad V, Tandon P, Singh GP, Maurya RP. Management of maxillary lateral incisor: Canine transposition along with maxillary canine impaction on the contralateral side. J Orthod Res [serial online] 2015 [cited 2018 Sep 6];3:61-4. Available from: http://www.jorthodr.org/text.asp?2015/3/1/61/146357 |
| Introduction | |  |
Transposition is a unique and extreme form of ectopic eruption in which permanent tooth develops and erupts in the position normally occupied by another tooth. According to Shapira and Kuftinec transposition is a relatively rare dental anomaly characterized by an interchange in the position of two permanent teeth on the same side of the dental arch. [1],[2] The maxillary canine is the tooth most frequently involve in the transposition. This can be divided into five types, which related to their distribution: [3]
- Canine - lateral incisor: 20%
- Canine - first premolar: 7%
- Canine - first molar: 4%
- Lateral incisor - central incisor: 3%
- Canine - central incisor: 2%.
The incidence of permanent canine impaction is approximately 2%, of which 80% are palatally impacted. However, amalgamation of impaction along with the transposition of maxillary teeth is very rare. The etiology of transposition is unclear. Various theories; such as genetic interchange in the position of developing tooth buds, [4],[5] lack of canine root resorption, mechanical interferences to erupting permanent tooth, early loss of deciduous tooth and prolong retention of deciduous tooth have been proposed to explain the phenomenon. In this case, the etiological factor for transposition and impaction of canine might be retained deciduous canine.
| Case Report | | |
A 24 years 5-month-old female reported with the chief complaint of irregularly arranged front teeth. The clinical examination revealed pleasing profile, Angles Class I molar relationship, maxillary right lateral incisor had erupted palatally in cross-bite along with distopalatal rotation and canine at the place of lateral incisor with mesiopalatal rotation (40°), while maxillary left deciduous canine was retained. [6] Her mesio-incisal edge of the right maxillary incisor was fractured due to trauma [Figure 1]a-g.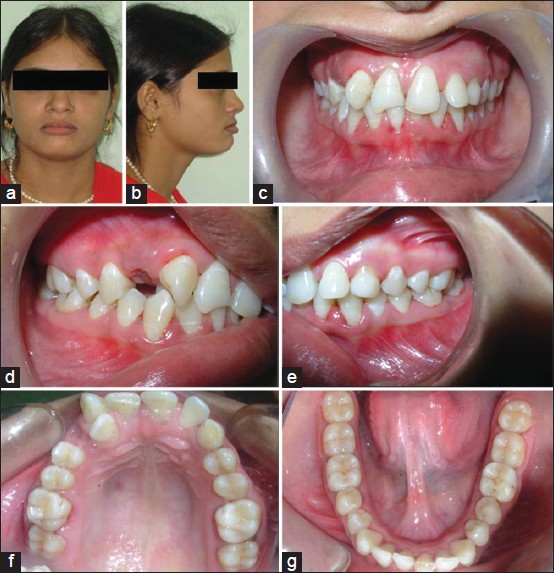 | Figure 1: Pretreatment Photographs. Extraoral: Frontal view (a) and profile view (b). Intraoral: frontal view (c), right lateral view (d), left lateral view (e), upper occlusal view (F) and lower occlusal view (g)
Click here to view |
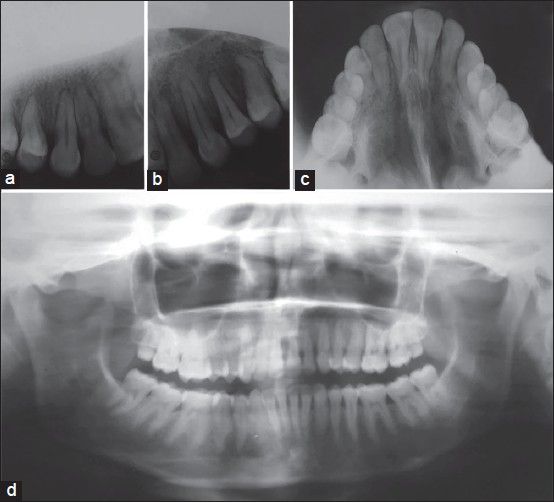
Intra oral periapical, occlusal, and orthopantomogram radiographs were taken. Radiographic examination showed that the maxillary canine and lateral incisor were fully transposed in the right side, while maxillary left canine was impacted along with retained deciduous canine. This maxillary canine-lateral incisor transposition was a kind of complete transposition because both crown and root were transposed [Figure 2]a-d.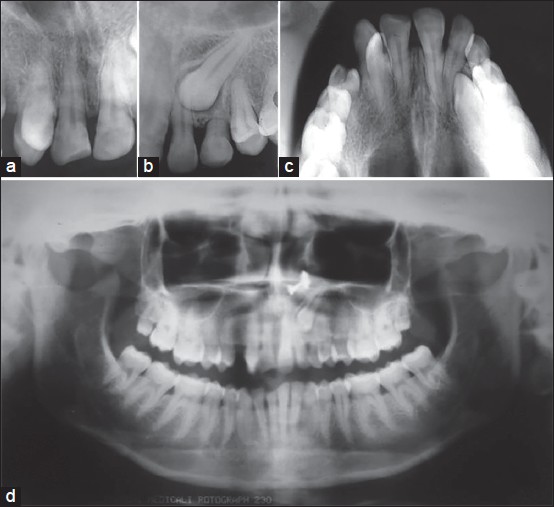 | Figure 2: Pretreatment radiographs. (a) Intra oral periapical (IOPA) X-ray showed complete transposition of maxillary right canine and lateral incisor. (b) IOPA X-ray showed impacted maxillary left canine and retained deciduous canine. (c and d) Occluasal and orthopantomogram radiographs showed complete transposition of maxillary right canine and lateral incisor and impacted maxillary left canine
Click here to view |
| Treatment Plan and Progress | | |
Transposed teeth should be aligned in their transposed positions, but when it affects the esthetics then another treatment approach should be considered where orthodontic movement of the teeth into their normal anatomic positions in the arch is required. It is easier to treat the transposed teeth in the early dentition period but it is quite difficult to treat in late permanent dentition period after the eruption of third molars. In this case, due to aesthetic reason it was decided to orthodontically move the teeth in their normal anatomical position in the dental arch.
The 0.022 × 0.028 slot maximal band tension appliance was placed on all teeth except right lateral incisor and left deciduous canine of maxillary arch. Since maxillary right canine was mesioangular rotated (approximately 40°) so, close coil spring was used to derotate and distal movement of canine simultaneously [Figure 3]a. For bodily movement of the canine the force was applied at the center of resistance using power arm which was fabricated by 0.016 × 0.022 stainless steel (SS) wire [Figure 3]b. Segment from right central incisor to left first molar of maxillary teeth were aligned and 0.019 × 0.025 SS stabilizing wire was placed. Posterior bite plate was fabricated and delivered to disocclude anterior teeth for correction of palatally displaced maxillary right lateral incisor. Initially, lighter force overlay wire was ligated to lateral incisor and gradually shifted to stiffer wire. Surgical exposure of impacted left maxillary canine and extraction of retained deciduous canine was done at the same time [Figure 4]a. Lingual button was bonded to impacted maxillary left canine, which was attached with 0.019 × 0.025 SS wire with the pig-tail tie [Figure 4]b. The closed eruption traction technique was used to provide good attached gingiva for erupted canine.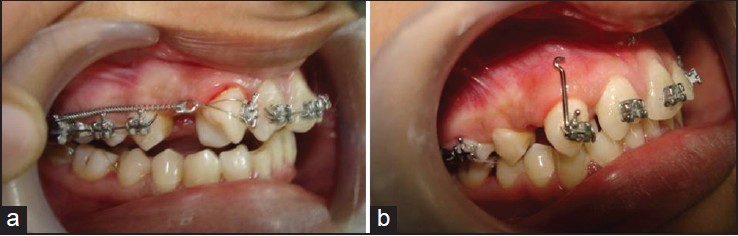 | Figure 3: Intraoral photograph showed use close coil spring for mesioangular rotation correction and distal movement of maxillary right canine (a) and power arm on maxillary right canine bracket, which coincides to the center of resistance and helps bodily movement of canine (b)
Click here to view |
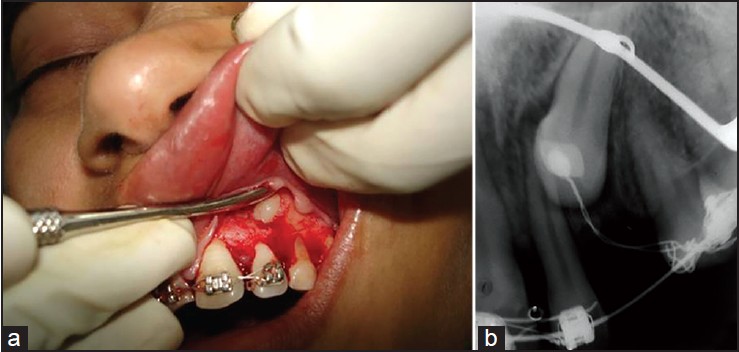 | Figure 4: (a) Surgical exposure of impacted maxillary left canine. (b) Intra oral periapical X-ray showing lingual button with pig-tail tie attached with 0.019 × 0.025 stainless steel arch wire
Click here to view |
When crown tip of the maxillary left canine get exposed in the oral cavity, bracket was bonded on the labial surface of the tooth and the auxiliary overlay wire was placed. Sequential change in the dimension of the wire was done until canine came in the proper alignment following the auxiliary. Overlay wire technique [7] was preferred which provide lighter force and simultaneously maintaining the arch integrity [Figure 5]a and b. | Figure 5: Mid treatment maxillary occlusal photograph (a) and occlusal radiograph (b)
Click here to view |
The maxillary arch was consolidated, 0.019 × 0.025 SS arch wire ligated and labial root torque was given for maxillary right lateral incisor. Finally, the fractured mesio-incisal edge of the maxillary right central incisor was restored by composite restorative material.
| Treatment Result | | |
Transposed right maxillary canine and lateral incisor as well as impacted left maxillary canine was well-aligned in the dental arch [Figure 6] and [Figure 7]. The total treatment time taken was 24 months, which was followed by a lingual-bonded canine-to-canine retainer. Vitality test was positive for both the canine and the lateral incisor and there was no root resorption was present at the end of treatment. Patient cooperation was excellent during the whole treatment procedures. | Figure 6: Posttreatment photographs. Extraoral: Frontal view (a) and profile view (b). Intraoral: frontal view (c), right lateral view (d), left lateral view (e), upper occlusal view (f) and lower occlusal view (g)
Click here to view |
 | Figure 7: Posttreatment radiographs. (a) Intra oral periapical (IOPA) X-ray showed well aligned transposed maxillary right canine and lateral incisor. (b) IOPA X-ray showed well aligned impacted maxillary left canine. (c and d) Occlusal and orthopantomogram radiographs showed well-aligned transposed maxillary right canine and lateral incisor and impacted maxillary left canine
Click here to view |
| Discussion | | |
The maxillary canines are keystones in the dental arch, both for aesthetics and normal masticatory function. Amalgamations of lateral incisor-canine transposition along with impaction were seen less often. Although many have speculated about the cause of transposition, it was recently determined that maxillary lateral incisor-canine transposition result from genetic influence in multifactorial inheritance model. The maxillary canine is more prone to deflect from its normal eruptive path by interfering obstacles than any other tooth in the dental arch. When deflected in lingual or labial plane, it may cause palatal or labial impaction and when displaced mesially or distally, it becomes transposed with lateral incisor or premolar respectively.
The clinical examination along with radiographic evaluation is used for early diagnosis of developing transposition and impaction. When detected early, interceptive treatment by removing etiological factor usually retained deciduous teeth may resolve the developing malocclusion. There are several treatment options including alignment of transposed teeth in their transposed position, extraction of one of the transposed teeth or orthodontic correction to their normal anatomic positions. Treatment plan depends upon patient's concern, esthetic and functional problems, but the best treatment is orthodontic positioning of the teeth in their respective position. If there are complete transposition of the maxillary canine and the lateral incisor, esthetics is the main concern to the patient and the parents. Therefore, alignment in their transposed position is not acceptable. Alignment of the transposed teeth in their normal position is probably best approach if possible.
| Conclusion | | |
The transposition along with impaction is the rare situation in the same arch. The treatment plan depends upon the patient and the parent concern about the esthetics, functional problems and also the degree of transposition whether it is complete or the incomplete. Preventive as well as early treatment in mixed dentition is the best time where we can easily correct the transposition whereas, in adult dentition period, where bone becomes denser and roots are completely formed causes difficulty in correction of transposition.
| References | | |
| 1. | Shapira Y. Transposition of canines. J Am Dent Assoc 1980;100:710-2.  |
| 2. | Shapira Y, Kuftinec MM. Tooth transpositions: A review of the literature and treatment considerations. Angle Orthod 1989;59:271-6. |
| 3. | Peck S, Peck L. Classification of maxillary tooth transpositions. Am J Orthod Dentofacial Orthop 1995;107:505-17. |
| 4. | Peck L, Peck S, Attia Y. Maxillary canine-first premolar transposition, associated dental anomalies and genetic basis. Angle Orthod 1993;63:99-109. |
| 5. | Chattopadhyay A, Srinivas K. Transposition of teeth and genetic etiology. Angle Orthod 1996;66:147-52. |
| 6. | Peck S, Peck L, Kataja M. Mandibular lateral incisor-canine transposition, concomitant dental anomalies, and genetic control. Angle Orthod 1998;68:455-66. |
| 7. | Cureton SL. The 'over and under' overlay wire. J Clin Orthod 1995;29:263-6. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7]
|










 Search Pubmed for
Search Pubmed for