|


 |
| CASE REPORT |
|
| Year : 2012 | Volume
: 4
| Issue : 1 | Page : 36-38 |
|
|
Laparoscopy-guided liver abscess drainage: An additional use of veress needle
Christopher N Ekwunife1, Ernest C Amadi1, Francis N Amaechi2, Ifeanyi C Ukaha3
1 Department of Surgery, Federal Medical Centre, Owerr, Nigeria
2 Department of Obstetrics and Gynecology, Federal Medical Centre, Owerr, Nigeria
3 Department of Works, Federal Medical Centre, Owerri, Nigeria
| Date of Web Publication | 5-Sep-2012 |
Correspondence Address:
Christopher N Ekwunife
Department of Surgery, Federal Medical Centre, Owerri
Nigeria
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.100352

 Abstract Abstract | | |
Percutaneous image-guided drainage is the standard of care in the treatment of liver abscess. However this may not suffice in multi-loculated abscesses and those associated with concomitant biliary pathology. We report the case of a 34 year old male who presented to our hospital with a huge hepatic abscess that could not be aspirated percutaneously. Subsequently he had a laparoscopic guided aspiration of the abscess, with the aid of veress needle. Three weeks post operatively, no residual abscess cavity was noticeable. We believe that minimal access surgery techniques should always be considered in the management of liver abscess, and that the veress needle can be an additional aspiration device, in our environment. Keywords: Liver abscess, laparoscopic surgery, veress needle
How to cite this article:
Ekwunife CN, Amadi EC, Amaechi FN, Ukaha IC. Laparoscopy-guided liver abscess drainage: An additional use of veress needle. J Surg Tech Case Report 2012;4:36-8 |
How to cite this URL:
Ekwunife CN, Amadi EC, Amaechi FN, Ukaha IC. Laparoscopy-guided liver abscess drainage: An additional use of veress needle. J Surg Tech Case Report [serial online] 2012 [cited 2016 Jun 10];4:36-8. Available from: http://www.jstcr.org/text.asp?2012/4/1/36/100352 |
| Introduction | |  |
The mainstay in the management of liver abscess has been the use of antibacterial agents and radiological guided percutaneous drainage. [1],[2] However, surgical intervention becomes necessary in the event of failed conservative therapy.
Open surgery is frequently done in our environment because of lack of standard equipment for percutaneous drainage. [3] This is associated with increased morbidity and mortality compared to percutaneous drainage. Consequently minimal access surgery techniques are increasingly being used in the treatment of this disease and various reports attest to the safety and better patient satisfaction with these procedures.
We report a case of laparoscopy-guided drainage of liver abscess in the process of which a veress needle was passed percutaneously to aspirate the abscess. This is the first reported case of use of laparoscopic technique in the treatment of liver abscess in Nigeria, to the best of our knowledge.
| Case Report | | |
A 34-year-old male commercial driver presented at the general surgery outpatient clinic of the Federal Medical Centre Owerri with a 3-week history of abdominal swelling and jaundice. There was a preceding history of diarrhea and vomiting but with no associated pruritus. Examination showed an emaciated man, pale, jaundiced and had bilateral pitting pedal edema. Abdomen was distended with a demonstrable ascites and a tender hepatomegaly. The blood pressure was 110/80 mm Hg, pulse rate 92 beats/min, and temperature 38.2°C.
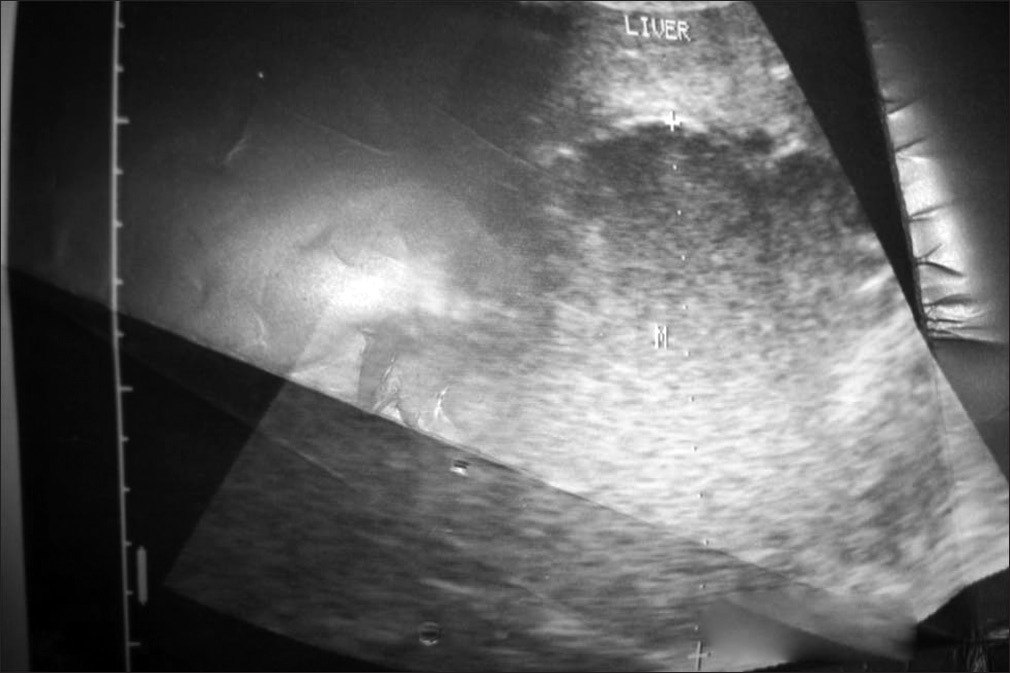
A provisional diagnosis of liver abscess was made and the patient was admitted into the ward. An abdominal ultrasound revealed an 11.6 cm abscess cavity located postero-superiorly in the right lobe of the liver. Hematologic investigation showed the following: hemoglobin 9 g/dl, white blood cells 20,200/mm3 (neutrophils 94%, lymphocytes 6%). The patient was started on intravenous metronidazole 500 mg 8-hourly and ceftriazone 2 g daily. Percutaneous aspiration of the abscess under ultrasound guidance was attempted but only 3 ml of purulent fluid was drained. The procedure was abandoned and patient elected to be discharged on antibiotics. A culture of the aspirated fluid yielded no bacterial growth. One week later, a repeat abdominal ultrasound revealed that the abscess cavity diameter has increased to 15.6 cm [Figure 1]. Then a decision was made to carry out a laparoscopic drainage of the abscess.
Carbon dioxide pneumoperitoneum was achieved with veress needle and thereafter three ports were inserted: 10 mm umbilical port for the camera; 10 mm subxiphoid and 5 mm right upper quadrant ports which were the working ports. Adhesions between the liver and diaphragm were freed with bipolar diathermy. Initially, we could not safely enter the abscess cavity safely with the hand instruments at our disposal (we had two graspers, a Maryland forceps and a needle holder) because it was not close to the liver surface from the view of our O° laparoscope. In order to avoid extensive trauma to the liver the veress needle was passed percutaneously (on the suggestion of our engineer) under direct vision from the right hypochondrium into the abscess cavity and 1500 ml of purulent fluid was aspirated. A peri-hepatic tube drain (size 24 F chest tube) was passed through the right hypochondrial port. The duration of the procedure was 2½ hours. Two days postoperatively, fever and the abdominal pain have subsided dramatically.
A repeat ultrasound done on postoperative day 3 showed that the abscess cavity has reduced to 5 cm. The tube drain was then removed and the patient was discharged home same day. At 3 weeks the abscess cavity has disappeared.
| Discussion | | |
Percutaneous drainage of liver abscess is the procedure of choice in the treatment of suppurative liver conditions. Surgery is usually reserved for selected cases such as those in which percutaneous option has failed or patients with large multiloculated abscesses containing thick pus or when underlying surgical pathology requires operation. [4],[5]
In this era of minimally invasive surgery, laparoscopic drainage of liver abscesses, combined with intravenous antibiotics, is a safe alternative for patients requiring surgical drainage when medical treatment has failed and in those with large abscesses. [2],[6],[7]
Our patient would have had open surgical drainage, when the image-guided abscess aspiration failed. The approach we adopted avoided the increased trauma and the prolonged hospital stay that would have resulted there from. We set out on a totally laparoscopic approach to the liver abscess drainage. This would have been facilitated if we had a greater range of instruments, including articulated hand instruments, at our disposal. However, in the process we discovered that a veress needle can be an effective tool for percutaneous aspiration of liver abscess.
Veress needle [Figure 2] is a spring-loaded 2 mm caliber device with a variable length of between 8 and 12 cm, which is used primarily to achieve pneumoperitoneum during laparoscopic surgery. It is also useful in laparoscopic port closure as well as ovarian cyst drainage. The veress needle is autoclavable and will be a cheaper alternative to standard disposable aspiration/drainage devices. Certainly, under ultrasound guidance the needle can be passed into the cavity without the need for laparoscopy. It will also be more effective than the use of intravenous cannula (which has been described in our region) [3] because of its bigger caliber and its longer length.
Drainage of liver abscess has also been done with laparoscopic trocar through which 28 French chest tube catheter was introduced. [8] However the veress needle is less traumatic; and when aspiration appears complete, drainage may not be routinely performed since there is often discomfort and morbidity associated with indwelling hepatic catheter. [1]
The duration of the procedure was unduly long because this was only the third laparoscopic surgery procedure we have been able to do in our hospital and we are not yet proficient in laparoscopic techniques. Also our experience shows the importance of team work as it was the engineer that actually suggested the use of the veress needle. It is hoped that our efforts will also encourage other surgeons in our sub region to take greater interest in laparoscopic surgery.
In conclusion, we suggest that the veress needle can be useful tool in the percutaneous aspiration of liver abscess.
| Acknowledgment | | |
This paper was presented at the 50 th Annual Conference of the West African College of Surgeons, Calabar, Nigeria on 9 th February 2010.
| References | | |
| 1. | Pearce NW, Knight R, Irving H, Menon K, Prasad KR, Pollard SG, et al. Non-operative management of pyogenic liver abscess. HPB (Oxford) 2003;5:91-5. 
[PUBMED] |
| 2. | Tay KH, Ravintharan T, Hoe MN, See AC, Chng HC. Laparoscopic drainage of liver abscesses. Br J Surg 1998;85:330-2.
[PUBMED] |
| 3. | Egba RN, Asuquo M, Ugare GU, Udoh I. Closed drainage of liver abscesses: The 'UNICAL' drain as an efficient and cost saving device in a tropical setting. Niger J Clin Pract 2008;11:396-9.
|
| 4. | Ferraioli G, Garlaschelli A, Zanaboni O. Percutaneous and surgical treatment of pyogenic liver abscesses: Observation over a 21- year period in 148 patients. Dig Liver Dis 2008;40:690-6.
|
| 5. | Ng SS, Lee JF, Lai PB. Role and outcome of conventional surgery in the treatment of pyogenic liver abscesses in the modern era of minimally invasive therapy. World J Gastroenterol 2008;14:747-51.
[PUBMED] |
| 6. | Wang W, Lee WJ, Wei PL, Chen TC, Huang MT. Laparoscopic drainage of pyogenic liver abscesses. Surg Today 2004;34:323-5.
[PUBMED] |
| 7. | Dominguez - Guzman DJ, Moreno - Portillo M, Garcia - Flores C, Blas - Franco M. Laparoscopic drainage of liver abscess. Initial experience. Cir Cir 2006;74:189-94.
|
| 8. | Kayaalp C, Yol S, Nessar G. Drainage of liver abscess via laparoscopic trocar with local anaesthesia. Surg Laparosc Endosc Percutan Tech 2003;13:121-4.
[PUBMED] |
[Figure 1], [Figure 2]
|