|


 |
| CASE REPORT |
|
| Year : 2012 | Volume
: 4
| Issue : 1 | Page : 32-35 |
|
|
Total laparoscopic management of a large renal hydatid cyst by using hydatid trocar cannula system
Saurabh Sudhir Chipde1, Abhishek Yadav1, Priyadarshi Ranjan1, Anand Prakash2, Rakesh Kapoor1
1 Department of Urology & Renal Transplantation, Sanjay Gandhi Post Graduate Institute of Medical Sciences (SGPGIMS), Lucknow, Uttar Pradesh, India
2 Department of Gastrosurgery, Sanjay Gandhi Post Graduate Institute of Medical Sciences (SGPGIMS), Lucknow, Uttar Pradesh, India
| Date of Web Publication | 5-Sep-2012 |
Correspondence Address:
Rakesh Kapoor
Department of Urology and Renal Transplantation, Sanjay Gandhi Post Graduate Institute of Medical Sciences (SGPGIMS), Lucknow - 14
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.100351

 Abstract Abstract | | |
Renal hydatidosis usually requires surgical treatment such as pericystectomy, marsupialization, or nephrectomy. In the era of minimally invasive surgery, laparoscopic treatment is preferred. Two main challenges in laparoscopy are to avoid the spillage of contents and to minimize incision for delivering the specimen. We herein discuss the use of a hydatid trocar cannula system (HTCS) to overcome these problems. A 46-year-old male patient having a large renal hydatid cyst (18×15 cm) was operated using HTCS. Three standard laparoscopic ports were placed and the HTCS was placed from the fourth port (18 mm). After aspiration of contents, the cyst was inspected using laparoscope and all contents were sucked. The operation time was 120 min and the total blood loss was around 100 ml. No intraoperative spillage was noted. The patient was orally allowed on Day 2 and discharged on Day 3. Oral albendazole therapy was continued 3 months after the operation. He remained symptom free and abdominal computed tomography did not reveal any recurrences during a follow-up of 2 years. Use of HTCS in renal hydatidosis not only prevents the spillage of hydatid fluid, but also assists in the complete evacuation of contents and allows intracystic visualization to check complete removal of scolices. Keywords: Hydatid disease, laparoscopy, renal
How to cite this article:
Chipde SS, Yadav A, Ranjan P, Prakash A, Kapoor R. Total laparoscopic management of a large renal hydatid cyst by using hydatid trocar cannula system. J Surg Tech Case Report 2012;4:32-5 |
How to cite this URL:
Chipde SS, Yadav A, Ranjan P, Prakash A, Kapoor R. Total laparoscopic management of a large renal hydatid cyst by using hydatid trocar cannula system. J Surg Tech Case Report [serial online] 2012 [cited 2016 Jun 10];4:32-5. Available from: http://www.jstcr.org/text.asp?2012/4/1/32/100351 |
| Introduction | |  |
Hydatid disease is endemic in Mediterranean countries, South America, and the Indian subcontinent. [1] Involvement of kidneys is rare and forms 2-4% of cases. [2],[3],[4],[5] Renal hydatid cysts primarily develop when the larvae, which are not filtered in the liver, pass through the pulmonary circulation and travel to the kidney. Commonly, it presents as chronic dull flank or lower back discomfort due to large size of cyst. It can also present with hydatiduria, ureteropelvic junction obstruction, and rarely as chronic renal failure when bilateral kidneys are involved. [6]
Medical therapy consists of albendazole alone or in combination with praziquantel by which cysts are sterilized. [7],[8] The World Health Organization (WHO) has recommended percutaneous aspiration, irrigation, and re-aspiration (the PAIR approach) for large liver hydatid cysts; [9] however, fear of anaphylactic shock resulting from spillage of hydatid fluid during treatment by this method may be discouraging a wider adoption of the technique. [10] A variety of surgical procedures have been advocated like pericystectomy, cyst marsupialization, and nephrectomy if the cysts are engulfing the entire kidney. In the laparoscopic era, the benefits of laparoscopy are extended to such patients. [11],[12] However, the major problem with large renal hydatid cysts is the spillage of contents during dissection and the extent of the incision for the delivery of specimen. In order to minimize spillage, every effort should be made to avoid rupture of the cyst while dissecting. This is difficult laparoscopically as the cysts are large and they have dense pericystic and perirenal adhesions. After dissection to deliver the specimen intact, the extent of incision is made large, so the patient is deprived of the benefits of laparoscopy. We describe the use of Hydatid Trocar cannula system which was originally designed for laparoscopic management of large hydatid cysts in the liver. [13]
| Case Report | | |
A 46-year-old man presented to the urology outpatient department with history of high-grade fever and dull aching left flank pain for the past 6 months. Abdominal examination revealed a large lump in the left flank. His total leukocyte count was elevated with an increase in the absolute eosinophil count. An ultrasonography of abdomen showed a large multilocular cyst replacing the left kidney, with floating membranes inside [Figure 1]a. A contrast-enhanced computed tomography (CECT) scan revealed the same findings without increase in enhancement or calcification of the cyst wall [Figure 1]b and c. Serum antibody test for hydatidosis was positive. The patient was given oral albendazole 400 mg twice daily for 4 weeks preoperatively. Then, a laparoscopic transperitoneal surgery was done using the hydatid trocar cannula system. | Figure 1: (a) USG showing multilocular hydatid cyst. (b and c) CECT showing left renal hydatid with multiple daughter cysts
Click here to view |
The Palanivelu hydatid trocar cannula system
The hydatid trocar cannula system consists of a 12-mm assembly of laparoscopic trocar and cannula along with 5-mm and 3-mm reducers. [13] The trocar is 29 cm long. It is fenestrated at the tip and hollow throughout its length to accommodate a suction cannula [Figure 2]. Its tip is pyramidal shaped, with each facet of the pyramid bearing a fenestration to enable any fluid leaking on its insertion to be sucked into its hollow body by the suction cannula placed within. Its long shaft also bears two fenestrations opposite to each other, at a distance of 17 cm from the tip. The cannula is 26 cm long with an inner diameter of 12 mm. It has two side channels, one for irrigation and another for suction [Figure 2] and [Figure 3]a. The suction channel has an inner diameter of 10 mm. | Figure 2: Palanivelu hydatid system consisting of a cannula and a trocar
Click here to view |
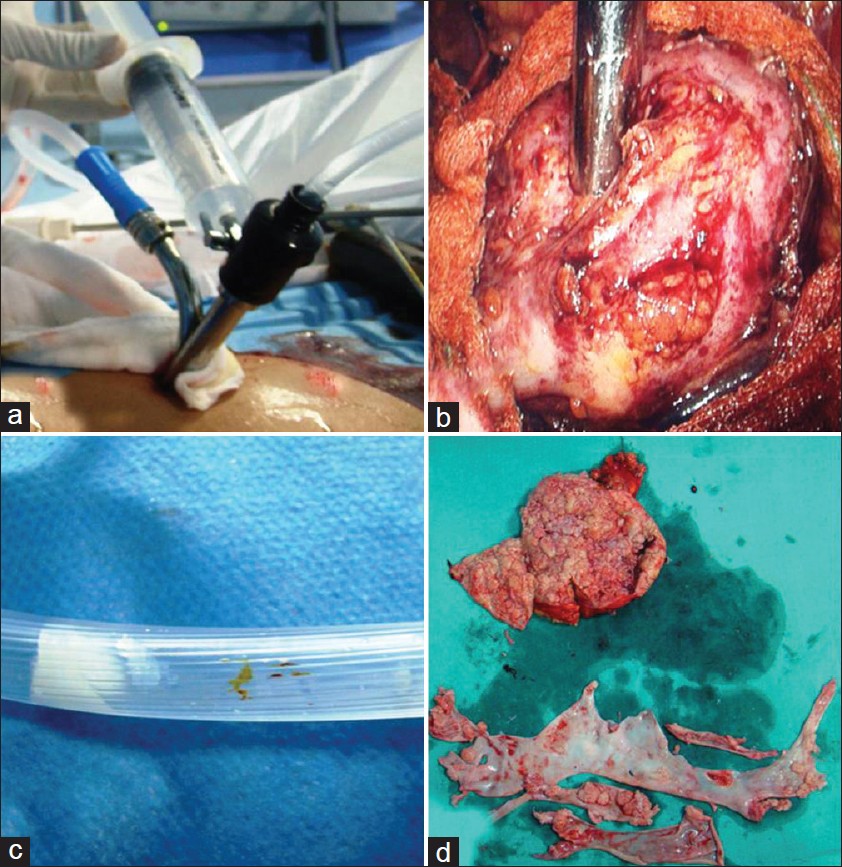 | Figure 3: (a) Palanivelu hydatid system outer cannula consisting of two side channels for suction and irrigation. (b) Intraoperative placement of PHS over the surface of hydatid cyst. (c) Hydatid scolices seen through suction tube. (d) Renal hydatid cyst cut opened after surgical removal with aspiratedscolices and laminated membranes
Click here to view |
Technique
For a left-sided renal surgery, left lateral position is made with a 60° tilt from the horizontal. Initially, three ports are placed; the first one is at the umbilicus (10 mm for the camera), the second is midway between the left anterior superior iliac spine and the umbilicus on the spino-umbilical line (10 mm, working port), and the third port is 2 cm below the rib margin in the left hypochondrium (5 mm, working port). The colon is mobilized and the renal area is dissected as in standard transperitoneal laparoscopic exposure for the kidney. The cyst is exposed all around by a combination of sharp and blunt dissection, especially near the tail of the pancreas, adrenal gland, and vessels. The cyst is isolated on all sides by packing it off using gauze pieces soaked with 10% povidone iodine, especially near the proposed site of introduction of the hydatid trocar and cannula, to minimize the spillage of the hydatid contents [Figure 3]b.
The Palanivelu hydatid system (PHS) trocar with cannula is introduced through the peritoneal cavity directly over the hydatid cyst via a 15-mm incision in the left flank. Once inside the peritoneal cavity, the trocar is removed and the cannula alone is advanced till its tip reaches over the surface of the hydatid cyst [Figure 3]b. At this stage, suction is applied through the side channel to maintain the contact between the cyst and the cannula opening. Thereafter, the fenestrated trocar with a 5-mm suction nozzle inside connected to another suction machine is introduced into the cannula and by a steady pressure it is introduced into the cyst. Care is taken to ensure that the suction is already switched on before the trocar is introduced in the cyst. At this level, utmost care is taken to avoid any spillage. Any fluid spillage on puncture of the cyst wall is immediately suctioned either into the body of the hollow trocar through its fenestrated tip and then into the suction cannula or into the outer cannula and then into the suction side channel. Once the PHS enters into the hydatid cyst, the trocar is removed and the cavity is irrigated with a scolicidal solution through the main channel while continuous suction is simultaneously maintained all the time. In this way, fragments of laminated membrane, daughter cysts, and debris are easily removed [Figure 3]c and d. Once the retaining fluid is clear, CO 2 is insufflated at low pressure (3-4 mm Hg) and the telescope is introduced into the cavity through the cannula to visualize the interior. After confirming the complete aspiration of cyst, hypertonic saline is instilled as the scolicidal agent for 10 min. After 10 min, the scolicidal agent is suctioned and the cyst is marsupialized or excised depending upon its location. Specimen is then retrieved through a specimen-retrieval bag and a thorough lavage is given in the peritoneal cavity with normal saline.
| Results | | |
The operation time was 120 min and the total blood loss was less than 100 ml. No intraoperative spillage was noted. The patient was orally allowed on Day 2 and discharged on Day 3. Oral albendazole therapy was continued 3 months after the operation. He remains symptom free and abdominal CT scan did not reveal any recurrences after 2 years of follow-up.
| Discussion | | |
Establishing a diagnosis and choosing the right treatment option for hydatid cysts of uncommon location such as the kidney can be a real challenge for the surgeon. Because of the lack of an absolutely effective systemic scolicidal agent, surgical treatment is the procedure of choice. Medical therapy in the form of oral albendazole is given for specific conditions like preoperative sterilization of widely disseminated hydatid disease, localized disease in poor surgical risk patients, ruptured cysts, and in patients in whom significant intraoperative spillage has occurred. [13]
Most of the renal hydatid cysts would require interventional or surgical treatment. A variety of surgical procedures are done for hydatid cysts disease, which are tailored to suit each individual case. These include marsupialization, closed total cystectomy, partial pericystectomy, and capitonnage with or without omentoplasty. [13] In the era of minimally invasive surgery, various laparoscopic procedures have been described to avoid the large incisions. The first report of laparoscopic treatment of hepatic hydatidosis was published in 1994. [14] Laparoscopic renal hydatid cyst treatments have been reported since 2006. [15] But these minimally invasive approaches have the problem of spillage and incomplete evacuation of the cyst contents.
The most important aspect while managing these cysts is avoidance of spillage. Rupture of an unsuspected hydatid cyst may lead to anaphylactic shock and there is also the risk of recurrence. In fact, an exaggerated fear of anaphylaxis seemed to discourage surgeons from more widely adopting laparoscopic techniques for the treatment of hydatid cysts. [16]
Few cases of retroperitonioscopic management of renal hydatidosis have been published with emphasis on measures to avoid spillage in peritoneum, but the problem with this approach is the small working field. [17],[18]
The other problem faced in laparoscopic treatment of hydatid cysts is the difficulty in evacuating the particulate contents of the cyst, the daughter cysts, and laminated membranes. Failure to remove all viable protoscolices in the initial operation may result in local recurrence. [19] Various instruments have been described to evacuate the contents of the liver hydatid cysts. Bickel et al. initially advocated the use of a large transparent beveled cannula. [20] Saglam described a perforator-grinder-aspirator apparatus designed specifically for the evacuation of hydatid cysts. [21] Kayaalp directly inserted a laparoscopic trocar into the hydatid cyst, but reported greater success for anterior and unilocular cysts only. [22] Al-Shareef et al. used a liposuction cannula to evacuate hydatid cysts. [23] Of all these, the isolated hypobaric technique described by Bickel et al. is the only one that has attempted to deal with the problem of spillage. PHS not only prevents any spillage of hydatid fluid, but also assists in complete evacuation of the cyst content and allows intracystic magnified visualization to check complete removal of scolices.
| Conclusion | | |
The hydatid trocar cannula system is highly effective in laparoscopic treatment of renal hydatid disease. It is optimum for preventing spillage and simultaneously evacuating the contents of hydatid cysts. With the use of this technique, the incision for delivering the specimen can be minimized, as the cyst is extracted after evacuation of its contents.
| References | | |
| 1. | Afsar H, Yagci F, Aybasti N, Meto S. Hydatid disease of the kidney. Br J Urol 1994;73:17-22. 
|
| 2. | Schantz PM, Schwabe C. Worldwide status of hydatid diseasecontrol. J Am Vet Assoc 1969;155:2104-21.
[PUBMED] |
| 3. | Horchani A, Nouira Y, Kbaier I, Attyaoui F, Zribi AS. Hydatid cyst of the kidney. A report of 147 controlled cases. Eur Urol 2000;38:461-7.
[PUBMED] |
| 4. | Kirkland K. Urological aspects of hydatid disease. Br J Urol 1996;38:241-54.
|
| 5. | Sarah JM, Christopher WJ, Warren DJ. Parasitic diseases of the genitourinary system. In: Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Campbell-walsh Urology. 9th ed. Philadelphia: Saunders; 2007. p. 458-9.
|
| 6. | Singh SK, Wadhwa P, Chandramohan V. Primary retrovesical hydatidosis causing chronic renal failure. Int J Urol 2006;13:76-9.
[PUBMED] |
| 7. | Nahmias J, Goldsmith R, Soibelman M, el-On J. Three-to 7-year follow-up after albendazole treatment of 68 patients with cystic echinococcosis (hydatid disease). Ann Trop Med Parasitol 1994;88:295-304.
[PUBMED] |
| 8. | Luchi S, Vincenti A, Messina F, Parenti M, Scasso A, Campatelli A. Albendazole treatment of human hydatid tissue. Scand J Infect Dis 1997;29:165-7.
[PUBMED] |
| 9. | Baijal SS, Basarge N, Srinadh ES, Mittal BR, Kumar A. Percutaneous management of renal hydatidosis: A minimally invasive therapeutic option. J Urol 1995;153:1199-201.
[PUBMED] |
| 10. | Yaghan R, Heis H, Bani-Hani K, Matalka I, Shatanawi N, Gharaibeh K, et al. Is fear of anaphylactic shock discouraging surgeons from more widely adopting percutaneous and laparoscopic techniques in the treatment of liver hydatid cyst? Am J Surg 2004;187:533-7.
[PUBMED] |
| 11. | Merdivenci A, Aydinlioglu K. Hydatidosis. Istanbul: University Publications of Medical Faculty; 1982. p. 440-59.
|
| 12. | Bilen CY, Ozkaya O, Sarýkaya Þ, Aþci R, Büyükalpelli R. Laparoscopic excision of renal hydatid cyst in a preadolescent. J Pediatr Urol 2006;2:210-3.
|
| 13. | Palanivelu C, Jani K, Malladi V, Senthilkumar R, Rajan PS, Sendhilkumar K, et al. Laparoscopic management of hepatic hydatid disease. JSLS 2006;10:56-62.
|
| 14. | Bickel A, Loberant N, Shtamler B. Laparoscopic treatment of hydatid cyst of the liver: Initial experience with a small series of patients. J Laparoendosc Surg 1994;4:127-33.
[PUBMED] |
| 15. | Rabii R, Mezzour MH, Essaki H, Fekak H, Joual A, Meziane F. Laparoscopic treatment for renal hydatid cyst. J Endourol 2006;20:199-201.
[PUBMED] |
| 16. | Yaghan R, Heis H, Bani-Hani K, Matalka I, Shatanawi N, Gharaibeh K, et al. Is fear of anaphylactic shock discouraging surgeons from more widely adopting percutaneous and laparoscopic techniques in the treatment of liver hydatid cyst? Am J Surg 2004;187:533-7.
[PUBMED] |
| 17. | Khan M, Sajjad Nazir S, Ahangar S,Farooq Qadri SJ, Ahmad Salroo N. Retroperitoneal laparoscopy for the management of renal hydatid cyst. Int J Surg 2010;8:266-8.
|
| 18. | Divarci E, Ulman I, Avanoðlu A, Retroperitoneoscopic laparoscopic treatment of renal hydatid cyst in a child. J Pediatr Surg 2010;45:262-4.
|
| 19. | Durakbasa CU, Tireli GA, Sehiralti V, Sander S, Tosyali AN, Mutus M. An audit on pediatric hydatid disease of uncommon localization: Incidence, diagnosis, surgical approach, and outcome. J Pediatr Surg 2006;41:1457-63.
[PUBMED] |
| 20. | Bickel A, Eitan A. The use of a large transparent cannula, with a beveled tip, for safe laparoscopic management of hydatid cysts of liver. Surg Endosc 1995;9:1304-5.
[PUBMED] |
| 21. | Saðlam A. Laparoscopic treatment of liver hydatid cysts. Surg Laparosc Endosc 1996;6:16-21.
|
| 22. | Kayaalp C. Evacuation of hydatid liver cysts using laparoscopic trocar. World J Surg 2002;26:1324-7.
|
| 23. | Al-Shareef Z, Hamour OA, Al-Shlash S, Ahmed I, Mohamed AA. Laparoscopic treatment of hepatic hydatid cysts with a liposuction device. JSLS 2002;6:327-30.
|
[Figure 1], [Figure 2], [Figure 3]
|
















