|


 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 6
| Issue : 2 | Page : 55-57 |
|
|
Transverse testicular ectopia with bilateral pyocoele: Case report and brief review of literature
Lokendra Kumar, Praveen Garg, ASN Rao, Ashish Kumar
Department of General Surgery, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India
| Date of Web Publication | 18-Dec-2014 |
Correspondence Address:
Lokendra Kumar
Department of General Surgery, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi 110 001
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.147260

 Abstract Abstract | | |
Transverse testicular ectopia (TTE) is a rare anomaly in which both testis descend through a single inguinal canal and enter to same hemiscrotum. To the best of our knowledge, we are reporting a new variant of TTE with right inguinal hernia with bilateral pyocoele. In this case, both testes descend separately through corresponding inguinal canal and present in single right scrotum. There is no report of bilateral orchidectomy for this variant of TTE with bilateral pyocoele with calcified necrosed testes. We also describe its embryology and management in brief, and review the previously reported cases. Keywords: Crossed testicular ectopia, transverse testicular ectopia, tunica vaginalis sac
How to cite this article:
Kumar L, Garg P, Rao A, Kumar A. Transverse testicular ectopia with bilateral pyocoele: Case report and brief review of literature
. J Surg Tech Case Report 2014;6:55-7 |
How to cite this URL:
Kumar L, Garg P, Rao A, Kumar A. Transverse testicular ectopia with bilateral pyocoele: Case report and brief review of literature
. J Surg Tech Case Report [serial online] 2014 [cited 2016 May 10];6:55-7. Available from: http://www.jstcr.org/text.asp?2014/6/2/55/147260 |
| Introduction | |  |
Undescended testes and testicular ectopia are two common anomaly of testes. Testes develop intraabdominally in retroperitoneal position and as the fetus grow up; it descends in to corresponding side of scrotum. Testes remain at the abdomen end of inguinal canal until 6 th month of intrauterine life. At 7 months it traverse the inguinal canal, at 8 th month reached at root of scrotum, and at 9 th month reaches in to scrotal sac. Arrest of its descent at any point along its normal pathway is called cryptorchidism, which may be either unilateral or bilateral or pass from external inguinal ring and deviate to one of these sites (Ectopia): Superficial inguinal pouch, femoral, contra lateral scrotum, pubic, penile and perineal areas. [1] Transverse testicular ectopia (TTE)/crossed testicular ectopia (CTE) is one of these categories. [2] In this rare congenital anomaly, both testis descend through a single inguinal canal and enter to same hemiscrotum. [2] Herein, we present a 65-year-old male patient with a new variant of TTE with bilateral pyocoele and brief review of literature.
| Case report | | |
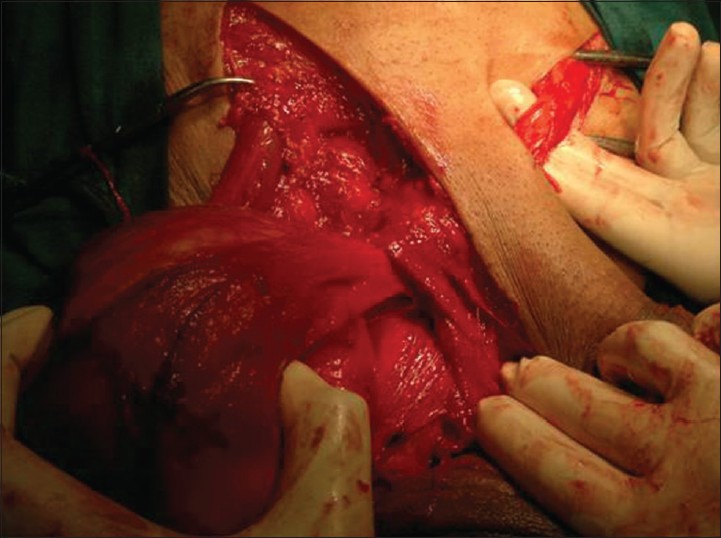
A 65-year-old male presented with complain of bilateral scrotal and right inguinal swelling for 3 years. Patient was examined and diagnosed as a case of bilateral pyocoele with right inguinal hernia with clinical suspicion of right testicular malignancy. On investigation, hemoglobin was 11.3 g/dl, total leukocytes count 5300/mm 3 , blood urea 30 mg/dl, serum creatinine 1.2 mg/dl and all other investigation including urine examination, liver function test and chest X-ray were reported normal. Tumor marker, beta human chorionic gonadotropin and serum alpha feto-protein were also reported in normal range. Operation was planned and an informed written consent was taken after explaining the disease and operative procedure. Consent of right orchidectomy was also taken. Patient was operated in supine position under spinal anesthesia. Right inguinal canal was opened and an indirect incomplete right inguinal hernial sac was found, sac was separated from the cord structure, and herniotomy was completed. Now, right testis was delivered from scrotum through right inguino-scrotal incision. After delivering of right testis, we noticed that there was another fluid filled sac in right scrotum [Figure 1]. Left scrotum was also full and contained a fluid filled sac creating intraoperative diagnostic dilemma. We checked all the possibilities and ruled out any herniation of gut loop into scrotum. To inspect the content, left inguinal canal was opened and spermatic cord was traced, which was crossing toward right scrotum above the root of penis in pubic region [Figure 2]. This was a new variant of TTE not classified before. Then we tried to separate out crossed left tunica vaginalis sac (TVS) containing left testis from right scrotum. Incidentally, the sac opened and dirty fluid material came out, which was suctioned [Figure 3]. As soon as the fluid was suctioned out, left scrotum was suddenly decompressed. Scrotal septum was incised and both crossed left TVS and left scrotal sacs [Figure 4] were delivered out and found a small communicating channel between the two. This situation was likely due to herniation of crossed left pyocoele sac into left scrotum and presented as bilateral pyocoele. To check the viability of testes, both testes were incised and found necrosed [Figure 5]. A second consent was taken intraoperatively for bilateral orchidectomy from patient and his relatives. After that bilateral orchidectomy and mesh hernioplasty was done. Suction drain was placed in both the scrotum and wound closed in layers. Scrotal drain was removed on fifth day and postoperative period was uneventful. The histopathological examination of section from hydrocele sac revealed dense fibro collagenous tissues with mild chronic inflammatory infiltrate. Focal areas showed cholesterol cleft with surrounding inflammatory infiltrate and calcification. Section from both testes revealed tubular sterosis with focal hyperplasia and chronic inflammatory infiltrate in interstitial tissue. Histological features were suggestive of chronic inflammatory lesion.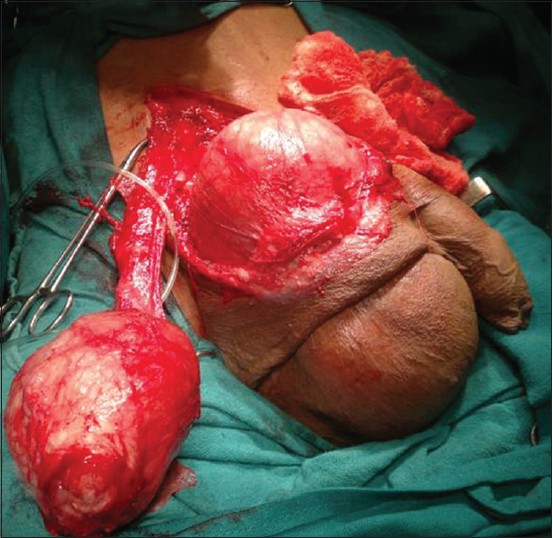 | Figure 1: Separated right cord and testes, left crossed ectopic testes with pyocoele and left scrotum
Click here to view |
| Discussion | | |
Normal testis almost always is located in the scrotum at birth; however, ectopic testis is located in the different sites including superficial inguinal pouch, suprapubic, femoral, perineal, base of penis, [1] and transverse ectopia. TTE is a rare form of testicular ectopia. It was first reported by Von Lenhossek in 1886. [3] Shamsuddin, Sarin, Nagdeve, and, recently, Naouar claimed that over hundred cases of TTE have been reported. [1],[4],[5] The oldest and youngest patients that have been reported in the literature were aged 77 years and 3 days, respectively. [2],[5] Several theories have been reported to explain the genesis of TTE. Berg [6] proposed the possibility of the development of both testes from the same genital ridge. Kimura [7] concluded that if both vasa differentia arose from one side, there had been unilateral origin but if there was bilateral origin, one testis had crossed over. Gupta and Das [8] postulated that adherence and fusion of the developing Wolffian ducts took place early, and that descent of one testis caused the second one to follow. On the basis of the presence of various associated anomalies, TTE has been classified into three types: Type 1, accompanied only by hernia (40-50%); type 2, accompanied by persistent or rudimentary Mullerian duct structures (30%); and type 3, associated with disorders other than persistent Mullerian remnants (inguinal hernia, hypospadias, pseudohermaphroditism, and scrotal abnormalities) (20%). Our case is a new variant not classified before and present as right indirect inguinal hernia with left CTE with bilateral pyocoele. Usually, the correct diagnosis is not made before surgical exploration, like our case, and it is revealed intraoperatively. The usefulness of radiologic evaluation in the detection of ectopic testis remains controversial. However, imaging of the scrotum in childhood is important. Sonography is the initial method of choice for localizing the testis and confirming the clinical findings. Computed tomography (CT) is not used frequently because of its radiation hazards. Magnetic resonance imaging (MRI) and MR venography [9] are excellent for the preoperative location of TTE. Patients with TTE are at increased risk of malignant transformation. In fact, the overall incidence of malignant transformation of gonads is 18%. [10] Once diagnosis of TTE is made, a conservative surgical approach in the form of orchiopexy is recommended for the preservation of fertility. Laparoscopy is useful for both diagnosis and treatment of TTE and associated anomalies. [11] Management for testicular ectopia is either transseptal or extra-peritoneal transposition orchiopexy. [12] In this case, the patient was aged 65 years and both the testes had no sign of viability, bilateral orchidectomy and mesh hernoplasty was done.
| Conclusion | | |
TTE is a rare anomaly of which the pathogenesis remains unclear, although a number of studies suggest that the gubernaculums may play an important role. Usually, the correct diagnosis is not made before surgical exploration and it is diagnosed intraoperatively. Currently, ultrasound and MRI are imaging modality of choice for preoperative evaluation and diagnosis. Laparoscopy is useful for both diagnosis and treatment of TTE. Orchiopexy is the treatment of choice, orchidectomy are performed rarely.
| References | | |
| 1. | Shamsuddin S, Mirza TH, Khan N, Ibrahim M, Imtiaz T. Transverse testicular ectopia. J Ayub Med Coll Abbottabad 2007;19:56-7.  |
| 2. | Debnath P, Tripathi R, Agarwal L, Malik E, Sharma S. Tuberculosis in Transverse Testicular Ectopic testis: A diagnostic dilemma: Case report. Indian J Tuberc 2006;53:27. |
| 3. | Von Lenhossek MN. Ectopia testis transversa. Anat Anz 1886;1:376-81. |
| 4. | Sarin YK, Nagdeve NG. Transverse testicular ectopia. Indian Pediatr 2005;42:293-4. [ PUBMED] |
| 5. | Naouar S, Maazoun K, Sahnoun L, Jouini R, Ksia A, Elezzi O, et al. Transverse testicular ectopia: A three-case report and review of the literature. Urology 2008;71:1070-3. |
| 6. | Berg AA. Transverse ectopy of the testis. Ann Surg 1904;40:223-4. [ PUBMED] |
| 7. | Kimura T. Transverse ectopy of the testis with masculine uterus. Ann Surg 1918;68:420-5. [ PUBMED] |
| 8. | Gupta RL, Das P. Ectopia testis transversa. J Indian Med Assoc 1960;16:35:547-9. |
| 9. | Lam WW, Le SD, Chan KL, Chan FL, Tam PK. Transverse testicular ectopia detected by MR imaging and MR angiography. Pediatr Radiol 2002;32:126-9. |
| 10. | Berkmen F. Persistent müllerian duct syndrome with or without transverse testicular ectopia and testis tumours. Br J Urol 1997;79:122-6. |
| 11. | Gornall PG, Pender DJ. Crossed testicular ectopia detected by laparoscopy. Br J Urol 1987;59:283. |
| 12. | Esteves E, Pinus J, Maranhão RF, Abib Sde C, Pinus J. Crossed testicular ectopia. Sao Paulo Med J 1995;113:935-40. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
|