|


 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 6
| Issue : 2 | Page : 58-60 |
|
|
Retrorectal cystic hamartoma: A problematic 'Tail'
Suhani, Kusum Meena, Shadan Ali, Lalit Aggarwal, Shaji Thomas
Department of General Surgery, Lady Hardinge Medical College and Smt. Sucheta Kriplani Hospital, Shaheed Bhagat Singh Marg, New Delhi, India
| Date of Web Publication | 18-Dec-2014 |
Correspondence Address:
Suhani
Senior Resident, Department of Surgery, Lady Hardinge Medical College and Smt. Sucheta Kriplani Hospital, Bhagat Singh Marg, New Delhi 110 001
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.147261

 Abstract Abstract | | |
The retrorectal space is an uncommon seat for neoplastic masses. Retrorectal hamartoma or tailgut cyst (TGC) is an uncommon developmental cystic lesion occurring in this space which mostly occurs in middle-aged females. We recently cared for a 16-year-old girl who presented with vague lower abdominal pain and occasional constipation. Per rectal examination revealed an extraluminal mass bulging from posterior rectal wall. Preoperative radiological investigations revealed by suggested it to be a mature cystic teratoma. The patient underwent exploratory laprotomy with en masse excision of the cyst. Histopathological examination of the specimen showed it to be a TGC. This case highlights the possibility of a TGC as a differential for retrorectal cystic lesions and the need to completely excise them given the possibility of future malignant transformation. Keywords: Presacral space, retrorectal hamartoma, tailgut cyst
How to cite this article:
Suhani, Meena K, Ali S, Aggarwal L, Thomas S. Retrorectal cystic hamartoma: A problematic 'Tail'. J Surg Tech Case Report 2014;6:58-60 |
How to cite this URL:
Suhani, Meena K, Ali S, Aggarwal L, Thomas S. Retrorectal cystic hamartoma: A problematic 'Tail'. J Surg Tech Case Report [serial online] 2014 [cited 2016 Jun 15];6:58-60. Available from: http://www.jstcr.org/text.asp?2014/6/2/58/147261 |
| Introduction | |  |
The retrorectal space is an uncommon area where tumors occur and these include primary tumors of neurogenic, osteogenic, and congenital origin; in addition to metastatic and inflammatory processes. Congenital lesions include chordomas (remnants of notochord), teratomas, anterior sacral meningoceles, and developmental cysts (dermoid, epidermoid, enteric duplication, and tailgut cysts (TGCs)). [1],[2] TGCs, also known as retrorectal cystic hamartomas, are a rare congenital lesion thought to arise from the remnants of the embryonic postanal gut. Hjermstad and Helwig were the first to publish their findings in 1988, and since then there have been no large case series reported. From review of the literature done by Killingsworth and Gadacz (keyword = tailgut cyst or retrorectal cystic hamartoma, limits = English), there have been 43 cases with confirmed diagnosis of TGC since their report. [3]
| Case report | | |
A 15-year-old girl presented with the complaints of lower abdominal pain and constipation occasionally. There was no history of bleeding per rectum or urinary complaints. She had attained menarche at 14 years of age and had normal menstrual cycle. General physical and per abdominal examination revealed no abnormal findings. However, on per rectal examination, there was a mass bulging from the posterior rectal wall, firm, and non-tender, with regular surface and smooth mobile rectal mucosa over it. An ultrasonogram (abdominal) revealed a large cystic lesion present in the left lower abdomen and the left ovary could not be seen separately. The patient then underwent a contrast-enhanced computed tomography (CECT) of the abdomen and pelvis which revealed a well-defined 12 × 13 × 9 cm multiseptated lesion in the presacral space which was pushing the rectum laterally and urinary bladder superiorly and abutting the sacrum and coccyx posteriorly [Figure 1]a and b]. The lesion was showing peripheral and septal calcification, few hyperdense nonehancing areas and few ossified fragments within it. Both ovaries were well-visualized separately. A provisional diagnosis of mature cystic teratoma was made and the patient underwent exploratory laparotomy wherein a large tubular tense cystic mass resembling fluid-filled intestinal loop filled with thick mucoid material was present in the presacral space [Figure 2]. The two ends of the tube were merging at the coccyx. The mass was displacing the sigmoid colon and rectum laterally and urinary bladder anteriorly. En masse removal was done.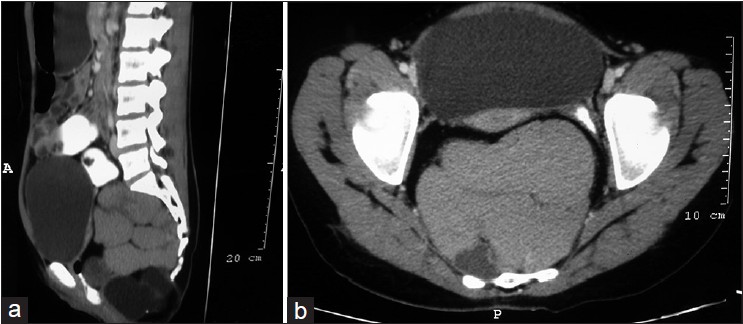 | Figure 1 (a and b): CECT abdomen showing multiseptated pre sacral mass compressing the rectum and displacing bladder superiorly
Click here to view |
 | Figure 2: Intraoperative picture showing a tubular fluid-filled structure displacing the bowel loops
Click here to view |
The patient had an uneventful postoperative recovery. The histopathological examination revealed it to be a retrorectal cystic hamartoma with areas of intestinal (large and small) and gastric epithelium. A solitary solid area within it had intestinal lining with area of squamous epithelial nests, haphazardly arranged muscle bundles, nerve bundles, and serous acini with few cystic spaces [Figure 3]a-c.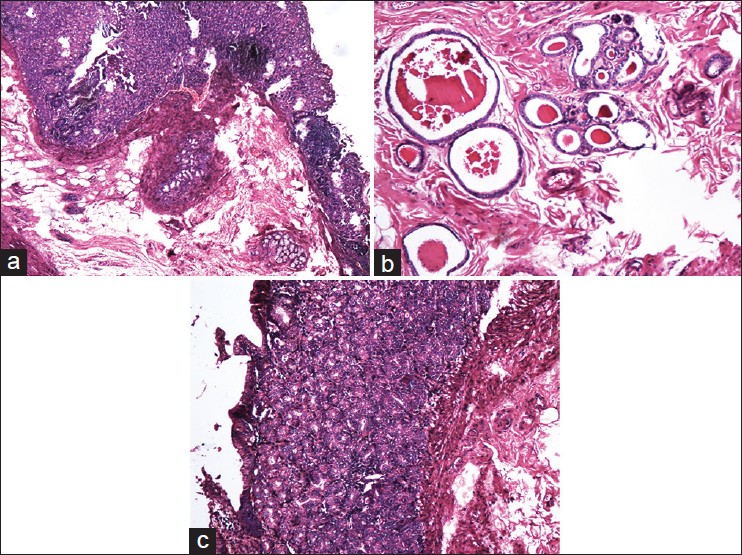 | Figure 3: Histopathological image showing (a) gastric mucosa, (b) ectopic gastrointestinal gland and (c) ectopic pancreatic epithelium
Click here to view |
| Discussion | | |
The retrorectal space is a potential space developed when a mass displaces the rectum anteriorly. It is formed posteriorly by the sacrum and coccyx and anteriorly by the rectum. The pelvic peritoneal reflection forms the superior border, and the levator ani and coccygeus muscles form the inferior border. The lateral boundaries consist of the ureters and iliac vessels. [4] The differential diagnosis of masses within this space is broad and includes primary tumors of neurogenic, osteogenic, and congenital origin; in addition to metastatic and inflammatory processes. Congenital lesions include chordomas, teratomas, anterior sacral meningoceles, and developmental cysts (dermoid, epidermoid, enteric duplication, and TGCs). [2] Excluding inflammatory lesions, developmental cysts are the most common masses in the retrorectal space. [1] TGCs are rare congenital lesions arising from remnants of normally regressing postanal primitive gut. They often present in middle-aged women with symptoms due to extrinsic rectal compression. Only one case of a retrorectal cystic hamartoma occurred in a 2-year-old child and very few cases have been reported in teen aged girls, as in our case. [3]
The differential diagnosis for a retrorectal mass can be narrowed using a combination of diagnostic tools to reach a preoperative diagnosis of a developmental cyst. Due to their location, almost all retrorectal tumors will be palpable on rectal examination, and developmental cysts will manifest as extrinsic masses. [1] Colonoscopy could rule out any rectal mucosal changes in cases of rectal bleeding. [1],[2] CT and magnetic resonance imaging (MRI) are useful imaging modalities that help in making a preoperative diagnosis. However, the definitive diagnosis and treatment is through complete surgical excision and pathological examination of the specimen. Preoperative biopsy should not be attempted (unless the mass is surgically unresectable at presentation) due to risk of spreading dysplastic cells through weakened cyst walls. In addition, tissue obtained from biopsy is often not extensive enough to show all the histology features necessary for diagnosis. [2],[5] Complete excision is necessary to prevent recurrence, infection, and possible malignant transformation. [6]
Developmental cysts are distinguished by their histopathologic differences. Dermoid and epidermoid cysts are both lined with stratified squamous epithelium; however, only dermoid cysts contain dermal appendages (hair follicles, sweat glands, and tooth buds). Dermoid cysts arise from faulty inclusion of ectoderm when the embryo coalesces. Epidermoid cysts are formed from inclusion of epidermal elements at the time of neural groove closure in the meninges. Rectal duplication cysts are lined by typical gastrointestinal epithelium (often with crypts, villi, and glands) and are surrounded by two well-formed layers of smooth muscle with nerve plexuses. TGCs, or retrorectal cystic hamartomas, are predominantly multicystic and can contain a variety of epithelia between cysts or even within the same cyst. Epithelial types include stratified squamous, transitional, mucinous or ciliated columnar, and cuboidal mucus secreting. In contrast to enteric duplication cysts, TGCs have disorganized smooth muscle fibers within the cyst wall and do not contain neural plexus. [5],[7]
| Conclusion | | |
Retrorectal hamartoma or TGC should be considered as a possible differential in any case of perirectal cyst, irrespective of age and gender. Complete surgical excision is of paramount importance due to reported risk of future malignancy.
| Acknowlegdement | | |
We would like to extend our heartfelt thanks to Dr. Manjula Jain, Head of pathology department, LHMC and SSKH for providing images of the histopathology slide for this case.
| References | | |
| 1. | Jao SW, Beart RW Jr, Spencer RJ, Reiman HM, Ilstrup DM. Retrorectal tumors. Mayo Clinic experience, 1960-1979. Dis Colon Rectum 1985;28:644-52.  |
| 2. | Hannon J, Subramony C, Scott-Conner CE. Benign retrorectal tumors in adults: The choice of operative approach. Am Surg 1994;60:267-72. |
| 3. | Killingsworth C, Gadacz TR. Tailgut cyst (retrorectal cystic hamartoma): Report of a case and review of the literature. Am Surg 2005;71:666-73. |
| 4. | Hjermstad BM, Helwig EB. Tailgut cysts. Report of 53 cases. Am J Clin Pathol 1988;89:139-47. |
| 5. | Prasad AR, Amin MB, Randolph TL, Lee CS, Ma CK. Retrorectai cystic hamartoma: Report of 5 cases with malignancy arising in 2. Arch Pathol Lab Med 2000;124:725-9. |
| 6. | Piura B, Rabinovich A, Sinelnikov I, Delgado B. Tailgut cyst initially misdiagnosed as ovarian tumor. Arch Gynecol Obstet 2005;272:301-3. |
| 7. | Dahan H, Arrivé L, Wendum D, Docou le Pointe H, Djouhri H, Tubiana JM. Retrorectal developmental cysts in adults: Clinical and radiologic-histopathologic review, differential diagnosis, and treatment. Radiographics 2001;21:575-84. |
[Figure 1], [Figure 2], [Figure 3]
|















