|


 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 6
| Issue : 2 | Page : 61-63 |
|
|
Aberrant right subclavian artery: A life-threatening anomaly that should be considered during esophagectomy
Rahim Mahmodlou1, Nariman Sepehrvand2, Sanaz Hatami1
1 Department of Surgery, Urmia University of Medical Sciences, Urmia, Iran
2 Department of Students' Research Committee, Urmia University of Medical Sciences, Urmia, Iran
| Date of Web Publication | 18-Dec-2014 |
Correspondence Address:
Nariman Sepehrvand
Department of Surgery, Imam Khomeini Training Hospital, Urmia University of Medical Sciences, Ershad Avenue, Urmia
Iran
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.147262

 Abstract Abstract | | |
Aberrant right subclavian artery (ARSA) is a rare anomaly, in which the right subclavian artery arises directly from the aortic arch instead of originating from the brachiocephalic artery. This anomaly should be taken into consideration during surgical procedures around esophagus, such as esophagectomy. Any unintentional injury of this artery during surgical procedures could be extremely life threatening. A 56-year-old woman presented with dysphagia, with concurrent aberrant subclavian artery and esophageal cancer. The transhiatal esophagectomy was performed successfully since the anomaly was preoperatively diagnosed using computed tomography scan. The presence of ARSA during esophagectomy may be challenging, but if diagnosed preoperatively, the precise and diligent dissection of the retroesophageal space during esophagectomy, may prevent any injury to the aberrant artery and consequent complications. Keywords: Aberrant subclavian artery, esophageal cancer, esophagectomy, lusoria
How to cite this article:
Mahmodlou R, Sepehrvand N, Hatami S. Aberrant right subclavian artery: A life-threatening anomaly that should be considered during esophagectomy. J Surg Tech Case Report 2014;6:61-3 |
How to cite this URL:
Mahmodlou R, Sepehrvand N, Hatami S. Aberrant right subclavian artery: A life-threatening anomaly that should be considered during esophagectomy. J Surg Tech Case Report [serial online] 2014 [cited 2016 May 10];6:61-3. Available from: http://www.jstcr.org/text.asp?2014/6/2/61/147262 |
| Introduction | |  |
Lusoria artery or aberrant right subclavian artery (ARSA) is a rare anatomical variation of the origin of the right subclavian artery. Essentially, right subclavian artery originates from the brachiocephalic artery, but in 0.4-1.8% of the general population it may arise directly from the aortic arch distal to the left subclavian artery. [1],[2],[3] ARSA on its way to the right arm crosses the midline posterior to esophagus.
The anomaly may be associated with some clinical manifestations such as dyspnea, stridor, dysphagia (which is called dysphagia lusoria), chest pain or fever, [4],[5],[6] but majority of cases with ARSA are asymptomatic.
Even if it is asymptomatic, this anomaly should be taken into consideration during surgical procedures around esophagus, such as esophagectomy. Any unintentional injury of this artery during surgical procedures could be extremely life threatening. In this article, we report the case of a patient with ARCA, who suffered concurrently from esophageal cancer.
| Case report | | |
The patient was a 56-year-old Caucasian woman, presented with the chief complaint of the dysphagia 3 months ago. Upper GI endoscopy revealed a mass in 30 cm from the incisors. A biopsy was taken from the mass, and the pathology was reported to be Squamous cell carcinoma. With the diagnosis of esophageal cancer, she underwent radiotherapy with 4500 rad in 25 fractions, and chemotherapy with 30 mg Cisplatin and 500 mg fluorourasil weekly for 4 week as neoadjuant chemotherapy. Three weeks after the last session of radiotherapy, she was scheduled for a transhiatal esophagectomy.
The thoracic computed tomography (CT) scan revealed that the patient has an ARSA behind the esophagus [Figure 1].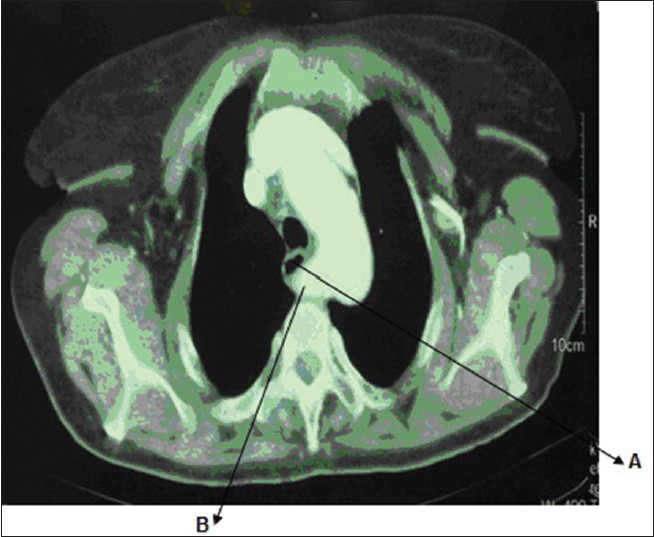 | Figure 1: Computed tomography scan of aberrant right subclavian artery (B) posterior to esophagus (A)
Click here to view |
In the operation, the upper abdominal incision from the bottom of the breastbone to the belly button is made. Gastrolysis was done, and the esophagus was freed up by working upward through the diaphragmatic hiatus. Another incision was made on the left side of the neck in the anterior border of the sternocleidomastoid. After sectioning the omohyoid and infrahyoid (strap) muscles and following the ligation of middle thyroid vein, the esophagus was exposed. Since the surgeon was aware of the presence of aberrant subclavian artery as a result of thoracic CT imaging, we did not dissect the posterior side of the esophagus bluntly, and the dissection was performed precisely, backward through the artery and forward through the trachea. The esophagus was separated using a Penrose drain [Figure 2] and the mediastinal dissection was done as a routine. The process of freeing up the esophagus was completed, and the esophagus was removed [Figure 3]. After closure of cardia, stomach was moved upward through the diaphragmatic hiatus into the chest (posterior mediastinum) until its upper end appeared in the site of the incision in the neck. The remaining esophagus is connected to the stomach in the neck. The cervical esophagogastic anastomosis was done between the remaining esophagus and the stomach using a gambee stitch.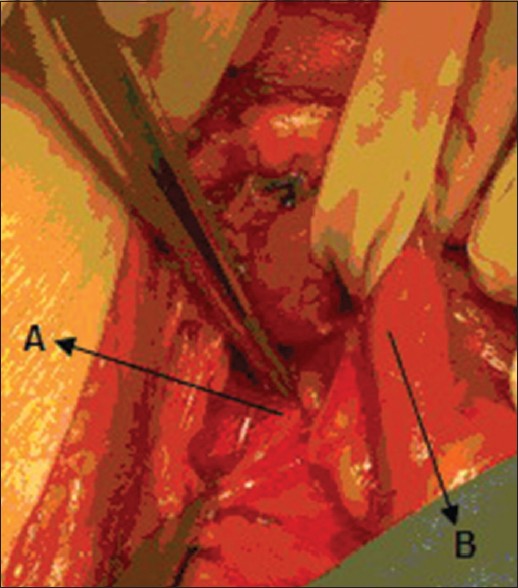 | Figure 2: Intraoperative photograph showing the aberrant right subclavian artery (A) in retroesophageal position, behind the esophagus (B) which is separated by Penrose drain
Click here to view |
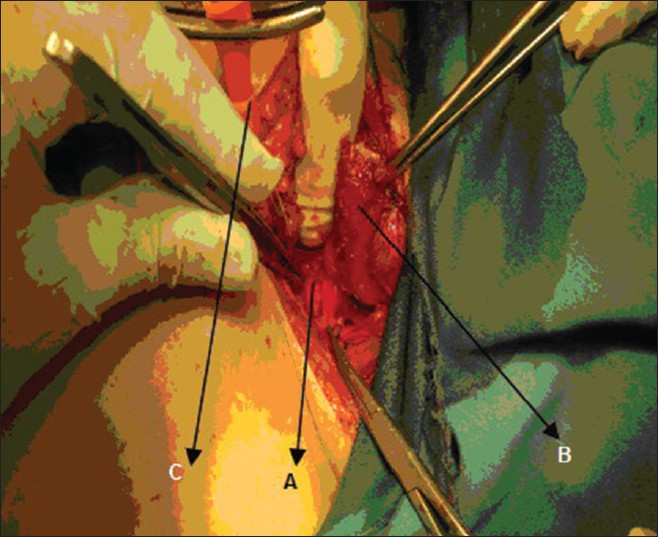 | Figure 3: Intraoperative view, (A) aberrant subclavian artery; (B) the stump of Esophagus; (C) nelaton catheter in posterior mediastinum after removal of esophagus
Click here to view |
Since the patient has not presented any sign and symptom related to the ARSA, and because of lacking any aneurysm in the origin of the aberrant artery, we have not treated the ARSA during the operation.
The surgery was eventless, and the patient was discharged from the hospital at the 7 th postoperative day. A 6 months follow-up demonstrated no problem or complication.
| Discussion | | |
Aberrant right subclavian artery is a rare phenomenon, but also the most common abnormality of the aortic arch. [7] Hanuld was first described this arterial anomaly in 1735, [6] but its symptomatic form was first described by Bayford in 1787 as the term of "dysphagia lusoria" or the freak of nature in patients with dysphagia. [8]
The anomaly is asymptomatic most of the time, but sometimes it's associated with various signs or symptoms, which the most frequent complaint among them is dysphagia. [1] Since the aberrant artery may pass the space between esophagus and vertebral column or the gap between esophagus and trachea in the midline, this anomaly may cause compression to the esophagus, which results in dysphagia. Three different conditions are speculated to play a role in presenting symptoms in ARSA: Stretching of the aberrant artery around the esophagus, becoming sclerotic and less plastic especially in elders, or being aneurismal. [5]
In the symptomatic cases, particularly in the cases with high-risk dilated aneurysm, the general census is advocating surgical treatment. [2],[5],[9] In asymptomatic cases, the anomaly has low importance, and there is no need for further intervention.
However in patients who are candidate for upper mediastinal interventions such as esophagectomy (especially the transhiatal esophagectomy), even the asymptomatic cases of this arterial anomaly become challenging.
First, if diagnosed early, the dysphagia resulted from a potential esophageal cancer may be attributed to dysphagia lusoria, and the patient may miss the appropriate treatment. In our case, despite the concurrency of ARSA with dysphagia, the rapid development of disphagia and also the result of esophagoscopy helped us to yield the diagnosis of esophageal cancer.
Furthermore in the presence of retro-esophageal right subclavian artery, right inferior laryngeal nerve will be abnormally nonrecurrent. Instead of recurring from the chest, it will pass directly from the vagus nerve at the level of the larynx to the neck. [10] This should be taken into consideration if a thyroid or parathyroid surgery is scheduled for any reason for the patient. [6]
Due to the proximity of the aberrant artery to the esophagus, if the ARSA was not identified preoperatively, any surgical procedure involving the esophagus without sufficient care may result in life-threatening issues. [11] The injury to the aberrant artery will cause mediastinal hemorrhage or even arterioesophageal fistula in long-term. [7],[12] Dissecting and mobilization of esophagus through cervical or transhiatal routes might pose a great risk of injury and complication on the aberrant artery if the surgeon was not aware of it.
There are reports that the surgeons had to change their technique of esophagectomy from transhiatal into transthoracic, since the anomaly was not diagnosed preoperatively, and the surgeons could not release the esophagus through the neck, [3] but other recent reports claimed that if the anomaly was identified and protected during the surgery, even transhiatal esophagectomy may be safely performed. [12]
For preoperative diagnosis of this anomaly several methods are suggested: Barium swallow may suggest the anomaly, especially in symptomatic patients. Noninvasive angiography methods (either CT or the magnetic resonance imaging) can be great confirmatory modality. [1],[2],[4],[6],[13] Multislice CT can diagnose this anomaly with high accuracy and also Esophagectomy may reveal a pulsatile impression in the posterior wall of the esophagus. [14]
| Conclusion | | |
The presence of an ARSA concurrent with esophageal cancer will pose a risk of injury during the procedure of esophagectomy, which should be considered by the surgeons and evaluated preoperatively through proper imaging studies.
| References | | |
| 1. | Dandelooy J, Coveliers JP, Van Schil PE, Anguille S. Dysphagia lusoria. CMAJ 2009;181:498.  |
| 2. | Hart PA, Kamath PS. Dysphagia lusoria. Mayo Clin Proc 2012;87:e17. |
| 3. | Pramesh CS, Saklani AP, Parmar V, Acharya S, Badwe RA. Aberrant subclavian artery causing difficulty in transhiatal esophageal dissection. Dis Esophagus 2003;16:173-6. |
| 4. | Abraham V, Mathew A, Cherian V, Chandran S, Mathew G. Aberrant subclavian artery: Anatomical curiosity or clinical entity. Int J Surg 2009;7:106-9. |
| 5. | Saeed G, Ganster G, Friedel N. Arteria lusoria aneurysm with truncus bicaroticus: Surgical resection without restoring blood supply to the right arm. Tex Heart Inst J 2010;37:602-7. |
| 6. | Saito T, Tamatsukuri Y, Hitosugi T, Miyakawa K, Shimizu T, Oi Y, et al. Three cases of retroesophageal right subclavian artery. J Nippon Med Sch 2005;72:375-82. |
| 7. | Pop D, Venissac N, Nadeemy AS, Schneck AS, Aze O, Mouroux J. Lesson to be learned: Beware of lusoria artery during transhiatal esophagectomy. Ann Thorac Surg 2012;94:1010-1. |
| 8. | Bayford D. An account of a singular case of obstructed deglutition. Mem Med Soc Lond 1794;2:271-82. |
| 9. | Myers PO, Fasel JH, Kalangos A, Gailloud P. Arteria lusoria: Developmental anatomy, clinical, radiological and surgical aspects. Ann Cardiol Angeiol (Paris) 2010;59:147-54. |
| 10. | Work WP. Unusual position of the right recurrent laryngeal nerve. Ann Otol Rhinol Laryngol 1941;50:769-75. |
| 11. | Lacout A, Khalil A, Figl A, Liloku R, Marcy PY. Vertebral arteria lusoria: A life-threatening condition for oesophageal surgery. Surg Radiol Anat 2012;34:381-3. |
| 12. | Temes RT, Tullis MJ, Lee P, Wernly JA. Transhiatal esophagectomy in a patient with aberrant right subclavian artery. Ann Thorac Surg 1999;68:2341-2. |
| 13. | Kent PD, Poterucha TH. Images in clinical medicine. Aberrant right subclavian artery and dysphagia lusoria. N Engl J Med 2002;346:1637. |
| 14. | Janssen M, Baggen MG, Veen HF, Smout AJ, Bekkers JA, Jonkman JG, et al. Dysphagia lusoria: Clinical aspects, manometric findings, diagnosis, and therapy. Am J Gastroenterol 2000;95:1411-6. |
[Figure 1], [Figure 2], [Figure 3]
|















